
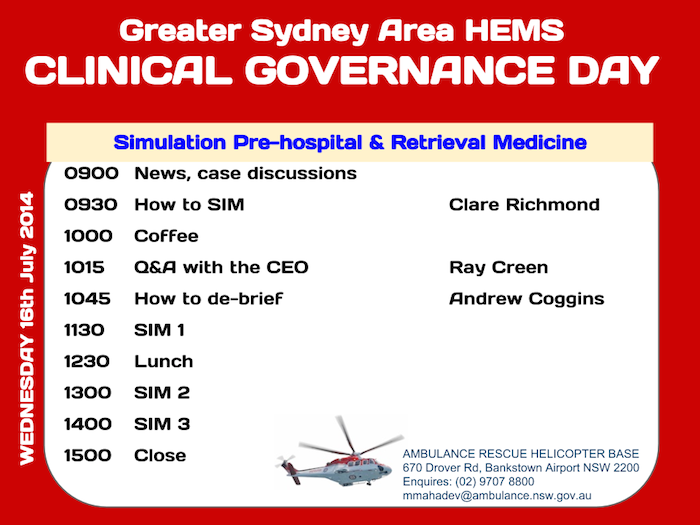
Here is the flyer for next week’s Clinical Governance Day.

Please note that as the training building is currently being refurbished, the CGD will instead be held in the conference room in the main office building (“The Castle”).
Here is the flyer for next week’s Clinical Governance Day.
Please note that as the training building is currently being refurbished, the CGD will instead be held in the conference room in the main office building (“The Castle”).
 The black swan theory describes rare events beyond the realm of normal expectation. We use ketamine on a daily basis, but are there any circumstances in which ketamine simply will NOT work?
The black swan theory describes rare events beyond the realm of normal expectation. We use ketamine on a daily basis, but are there any circumstances in which ketamine simply will NOT work?
This interesting case report by an Ex-Sydney HEMS physician Daniel Kornhall describes how ketamine failed completely as an anaesthetic agent in a psychiatric patient with a toxic lamotrigine overdose.
Lamotrigine, as we all obviously know, exerts its antiepileptic effect by inhibiting presynaptic sodium channels thus reducing the release of the excitatory glutamate and stabilising excitable neuronal membranes. Ketamine’s dissociative anaesthetic effects are a bit more of a mystery and diverse, but they are thought to involve increasing glutamate release through non-NMDA receptor pathways. It therefore follows, that if one drug prevents the release of glutamate and second drugs effects depend on its release, the second drug will not work.
With our high volume of ketamine use, incidents such as this are worth bearing in mind the next time you see a patient with a mixed polypharmacy overdose.
Lamotrigine is therefore ketamine’s black swan.
Fascinating talk on the development of this resuscitative technology by Dr Jim Manning who appeared in person at our Clinical Governance Day.
For further information check out EMCrit Podcast Episode 123

Several of our consultants are presenting at the Developing EM conference in Brazil. If you’d like to hear more, organising emergency physicians and prehospital & retrieval medicine consultants Mark Newcombe and Lee Fineberg describe it and also discuss the highly successful Developing EM conference they ran last year in Cuba:
Check out the program and register here
The project is a not-for-profit venture and no SydneyHEMS specialist receives financial remuneration for involvement in the DevelopingEM conference.

See here for directions
 “Don’t train and prepare until you get it right. Train and prepare until you can’t get it wrong.”
“Don’t train and prepare until you get it right. Train and prepare until you can’t get it wrong.”
Sydney HEMS is proud to be given permission to share Michael Lauria‘s talk on Cognition and Decision Making Under Stress. Training in medicine and working as a flight paramedic with the Dartmouth-Hitchcock Advanced Response Team, Michael has extensive military combat experience with special forces and is ideally placed to share thoughts and experience on how to prepare for and execute challenging missions.
His five take home points are:
You can download the audio file by right-clicking here
If you’d like to see the accompanying slides the talk can be viewed on YouTube
Audio made available thanks to our mate EMCrit
One of our own Sydney HEMS physicians is an extreme environment and mountain medicine expert – Dr Yashvi Wilamasena. Yash, as he is known to his mates, plans to reach the summit of Everest in the near future. In preparation for this he was there earlier this year. It was, of course, a fateful climbing season when an avalanche claimed the lives of 16 and severely injured 9. Whilst working in the Everest Basecamp ER, Yash, along with Sydney HEMS colleague Dr Jan Trojanowski recorded a series of videocasts that take us through the significant challenges of emergency medicine at 5,000 metres. Here’s the first:
Check out the inspiring Adventure Medic site for more sharp-end-of-the-sharp-end-of-medicine stuff, and where you’ll be able to view the remainder of the Extreme Medicine episodes as they’re published
Inspired by Roger Harris and Craig Hore’s escharotomy training video, we have created our own escharotomy model for HEMS physician training.
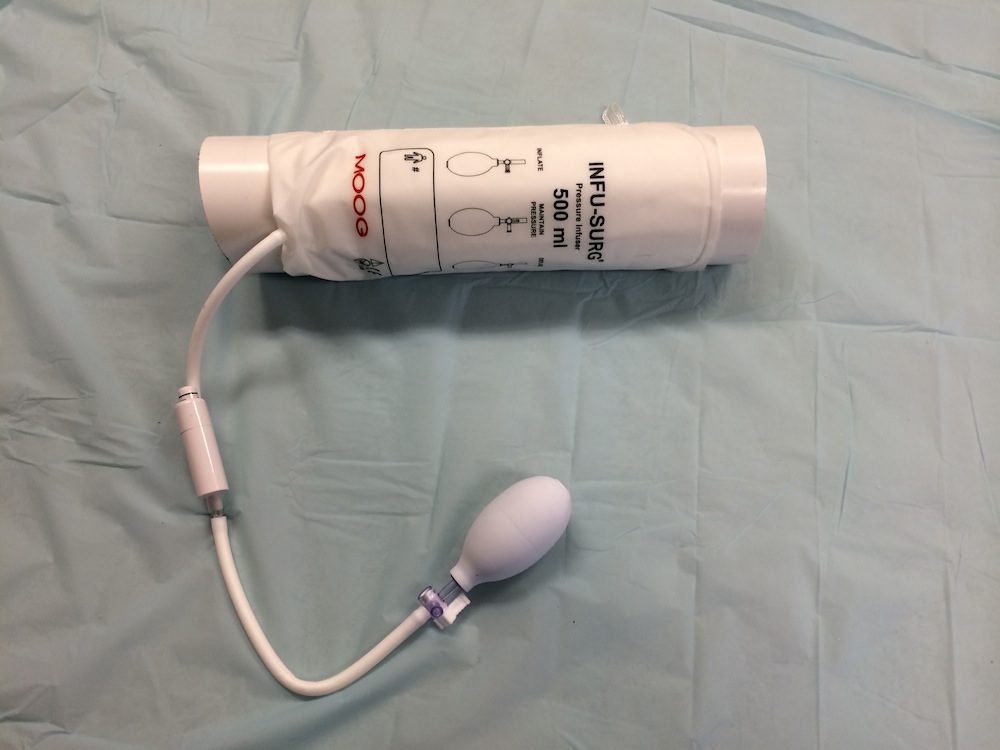
Our model is based on Roger Harris’ original design with a few minor modifications. With the exception of the arterial line pressure bag, all items were sourced from Bunnings hardware store and the local supermarket. The whole thing takes about five minutes to assemble.
Ingredients:
Fig 1 – Arterial line pressure bag and PVC pipe

Fig 2 – Glad-wrapped piece of meat to simulate muscle

Step 1
Wrap the arterial line pressure bag around the length of PVC pipe.
Step 2
Wrap a layer of Glad Wrap around the pipe. This will protect it from being contaminated by the overlying meat layer.

Step 3
Using Glad Wrap, bind the “muscle” onto the pipe, ensuring that it lies directly on top of the pressure bag.

Step 4
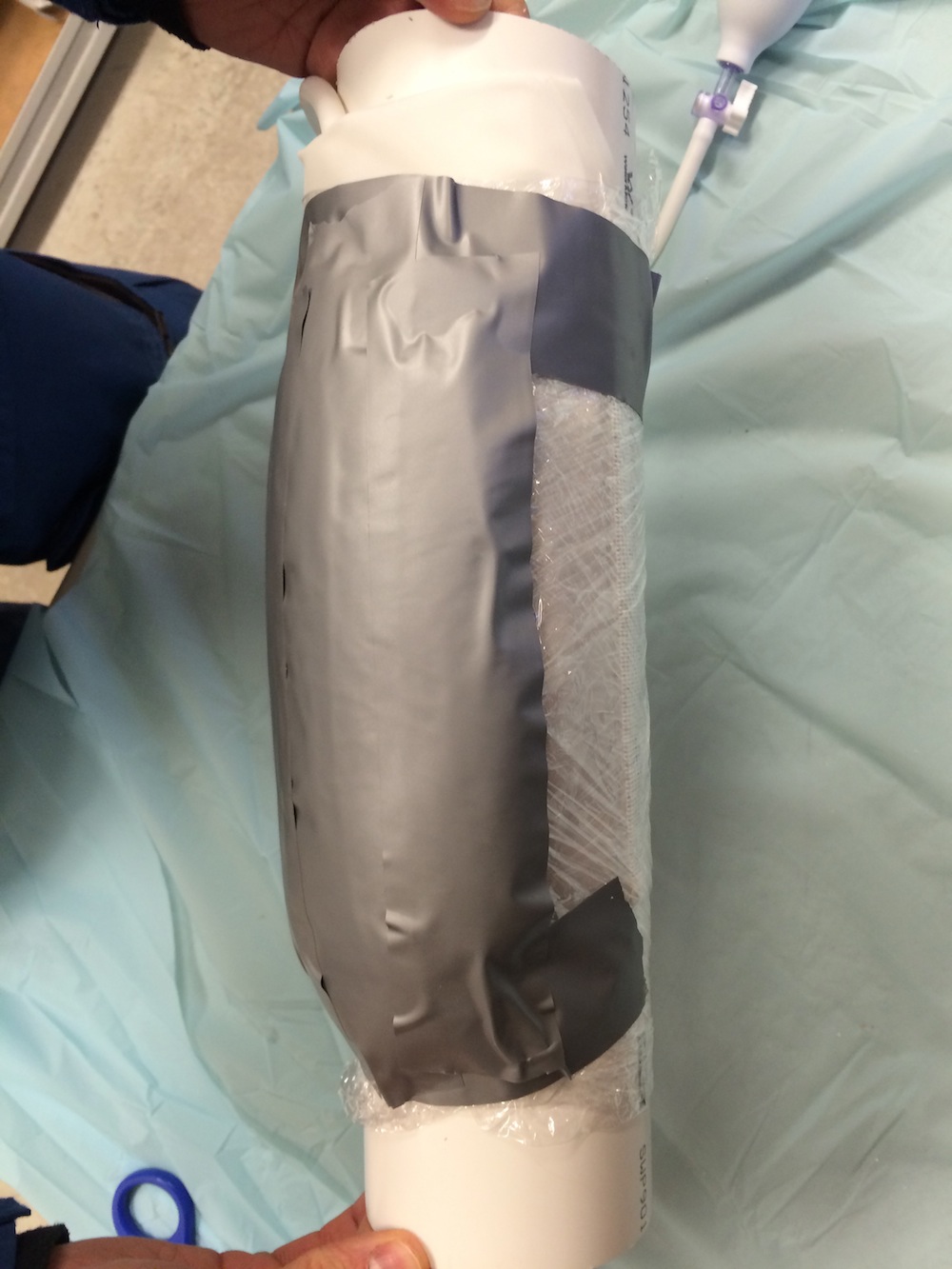
Secure the meat with circumferential straps of silver duct tape.

Step 5
Add a longitudinal layer of silver duct tape to simulate the deep fascia.
Step 6
Fold the foam packing material around 6-8 sheets thick and apply on top of the deep fascia layer to simulate subcutaneous fat.

Step 7
Secure the foam using the white Gaffer tape, which doubles up as the skin / eschar layer.

In this case, a hollowed-out glove box has been used as a base for the model. For greater realism, the limb could be attached to a mannequin.
Step 8
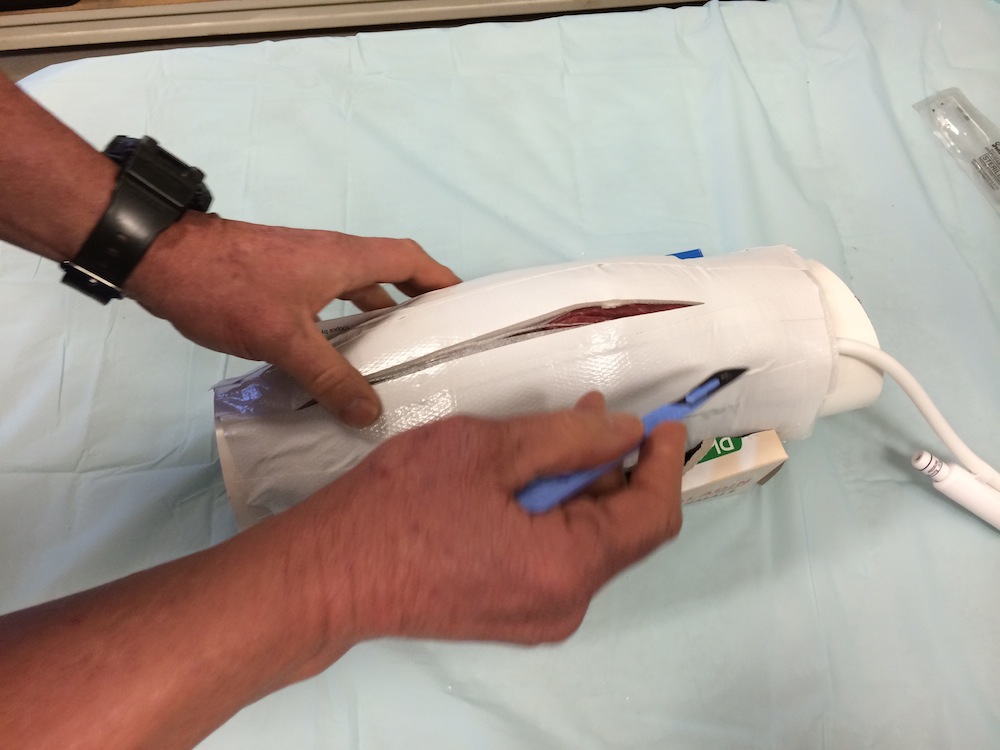
Pump up the pressure bag. This simulates tense oedematous soft tissues and will cause the skin layer to spring apart with a “pop” when incised.
Step 9
Cut the skin!
Step 10
Skin layer can be repaired for re-use by applying additional layers of white Gaffer tape.
If anybody has any bright ideas on how to replace the meat layer with something less organic, please comment below!
Escharotomy model MK II designed by Ed Burns, Craig Hore and Cliff Reid based on original design by Roger Harris.
Links
Chris Nickson’s guide to escharotomy from LITFL
Craig Hore explains escharotomy
 A decade ago simulation was a small part of the learning sphere but in the modern day of medical education it is now becoming commonplace and a somewhat essential part of training. With its embrace, particularly in the field of critical care, comes the evolution of the equipment, science and methodology.
A decade ago simulation was a small part of the learning sphere but in the modern day of medical education it is now becoming commonplace and a somewhat essential part of training. With its embrace, particularly in the field of critical care, comes the evolution of the equipment, science and methodology.
We had the good fortune of having the SiLECT team from Westmead starring Andrew Coggins and Mahesh together with GSA-HEMS’ own sim guru Clare Richmond, providing us with some pearls in how to run simulation and most importantly how to use the de-brief to learn and enquire. Continue reading
Here is the program for 16th July 2014, when we’ll have simulation experts Andrew Coggins and Clare Richmond – both emergency and retrieval physicians with extensive simulation experience – taking us through our paces on how to sim.
See here for directions
The following articles are recommended for pre-reading:
Back to the Basics in Medical Simulation: 11 Programmatic Factors from Academic Life in EM
Writing a Medical Simulation Case also from Academic Life in EM
Medical Education – Advocacy and Enquiry In a Nutshell from EmergencyPedia

