Drowning is an all too common cause of morbidity and death, particularly in a region as rich in water activities as New South Wales. Providers of prehospital critical care should seek to master drowning management, as it is one of the conditions where early interventions in the field can save a life.

This post is not intended to be a comprehensive overview of drowning, but an effort to share lessons learned, and knowledge refined, subsequent to some experience in the field.
Patients don’t necessarily stay “Dead or OK” – Dogma suggests that on our arrival, drowning victims are rescued on either extreme of the clinical spectrum, and remain that way. In the brief interval of a water winch rescue and landing on a nearby headland, our institutional experience suggests this is true. However, when on scene for a longer period of time, there is no way to predict how the clinical picture will change. The literature looking at survival outcomes is important, but it doesn’t help with the patient in front of you. Maintain a high level of suspicion for developing badness, and (mentally, at least) prepare for deterioration.
Optimize oxygenation with PEEP and FiO2 – Hypoxia is the crux of drowning pathophysiology; as such, it is essential to focus on improving oxygenation (and ventilation) early. Optimize oxygenation with increasing FiO2 and PEEP. Goal sats: mid-90s. In awake patients, you can support breathing by BVM with PEEP valve, or NIV. When intubated, consider a rational approach for FiO2 and PEEP changes, such as this table from ARDSnet Note how high you can go up on the PEEP, if needed.
![ScreenClip [4].png](https://sydneyhems.com/wp-content/uploads/2016/03/screenclip-4.png?w=640)
Beware the pulse ox readings – Ironically, even though oxygenation is essential, the pulse oximeter may not be very reliable in drowning patients. In a study of healthy volunteers, up to 50% of pulse oximetry readings were “spurious” after a 10 minute swim in cold water. Cold and poor perfusion are well-known spoilers of pulse ox traces. Additionally, by nature of their algorithms, pulse oximeters are only rated to be accurate above 70%, including the finger probe in our monitoring pouch and the new Zoll X Series. With a reading <70%, the machine is basically guessing. 
Ventilate drownings like ARDS patients – Although not formally studied, expert consensus suggests a lung protective ventilator strategy for intubated drowning patients. Use low tidal volumes (6ml/kg IBW) coupled with higher respiratory rates, low plateau pressures, and permissive hypercapnea (if head injury not a concern). Life In The Fast Lane has an excellent blog post about mastering our ventilator, including some cheat sheets for this strategy: Own The Oxylog 3000
Share your mental model – We should not only have open and constant communication within our doctor-paramedic team, but also with the other crews involved. Each views the same scene colored by different goals, priorities, and perspectives. When a situation changes or is increasingly intense, you should be extra cognizant of the potential for communication breakdown.
Worthwhile Reading Not Linked Above
- Garner AA, Barker CL, and Weatherall AD. Retrospective evaluation of prehospital
triage, presentation, interventions and outcome in paediatric drowning managed
by a physician staffed helicopter emergency medical service. Scand J Trauma Resusc Emerg Med. 2015; 23:92.
- Martinez FE and Hooper AJ. Drowning and immersion injury. Anaesth Intensive Care. 2014; 15(9):420-423.
- Szpilman D, Bierens JJ, Handley AJ, and Orlowski JP. Drowning. N Engl J Med. 2012; 366(22):2102-10.
- Topjian AA, Berg RA, Bierens JJ, et al. Brain Resuscitation in the Drowning Victim. Neurocrit Care. 2012; 17:441–467.
- Truhlar A, Deakin CD, Soard J, et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 4. Cardiac arrest in special circumstances. Resuscitation. 2015; 95:148–201. (Drowning is 174-176)

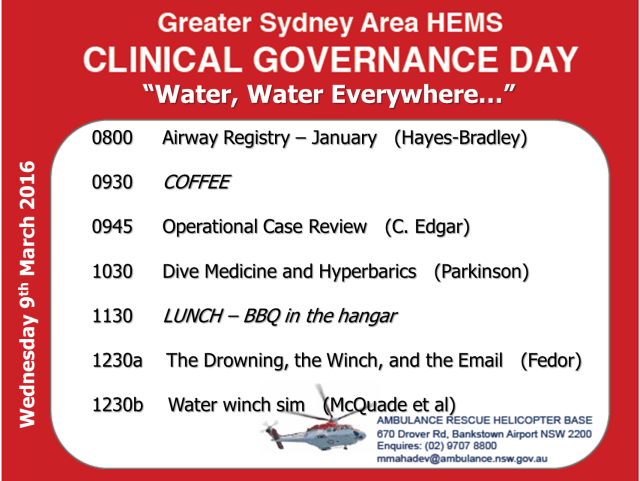 The next Clinical Governance Day will be on 9th March. This session is designed to be operationally focused and give you pearls and tools to use on your next shift. Thematically, we will be focusing on water-related topics.
The next Clinical Governance Day will be on 9th March. This session is designed to be operationally focused and give you pearls and tools to use on your next shift. Thematically, we will be focusing on water-related topics.