Our next Clinical Governance Day is on 5 October 2016 from 0800-1400.
Dr Albert Chiu (Interventional Neuroradiologist at Prince of Wales) will be kindly joining us and presenting on the latest developments in clot retrieval for hyperacute stroke.
A multidisciplinary team will be presenting a recent challenging fixed wing case with multiple decision points both logistical and medical. Full audience participation will be required so we will endeavour to avoid a repeat of the great coffee drought of 21/9.
There will be the regular offerings of Morbidity and Mortality with Airway Registry after lunch. A BBQ lunch will be available in the hangar.
All NSW Health staff are welcome to attend, a sign in is required. See here for directions: https://sydneyhems.com/contact.
Join us next Wednesday for a human-factors-focused clinical governance day at the Bankstown helicopter base.
We are particularly excited to welcome Paul Mayer, a Naval medic who returned from operational duties in Afghanistan earlier this year. He’s going to talk about his experiences of human factors in combat along with his reflections on how the Sydney HEMS induction course (which he attended in 2014) helped prepare him for delivering care on the frontline.
We’ll be undertaking an interactive exploration of some recent challenging cases from the service and taking time to learn from excellence in our HEMS practice (formally known as ‘Awesome and Amazing’).
We’re hoping to take a break for a BBQ lunch in the hangar before rounding off the day by putting our thoughts into action with some simulation.
As always, all NSW Health staff are welcome to attend, a sign in is required. See here for directions: https://sydneyhems.com/contact.
Next week’s CGD will include a review of June’s Mortality & Morbidity as well as the Airway Registry.
We will also hear from Mark Newcombe’s recent first hand experience of the Advanced Airway HOP. How would you have approached this difficult intubation in the middle of the night?!
Keeping things light hearted but always educational, there will be an end of term quiz (with prizes!).
As another 6 month term draws to a close, we would like to thank this fantastic registrar group for all your hard work and commitment. If you are leaving us in August then we wish you all the best in your next endeavours and if you are staying then we look forward to an action packed next term!
As always, all NSW Health staff are welcome to attend, a sign in is required. See here for directions: https://sydneyhems.com/contact/
Retrieval medicine specialist Dr Stefan Mazur outlines postgraduate academic study options for retrieval clinicians. As he points out, the list is not exhaustive, and focuses on Australasian and British courses and exams.
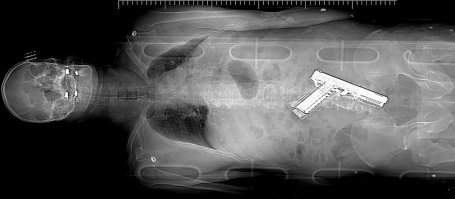
Our Clinical Governance Day on 15 June 2016 was an introductory discussion about the why, who, and how of tactical medicine. Out of this came a recognition of the importance of this knowledge base and skill set not only for the next Lindt Cafe Siege or other high threat event, but also for our daily trauma practice. This is a summary of the highlights as well as some additional key concepts.
THE #1 RULE OF TACTICAL MEDICINE IS… 1st WIN THE GUN FIGHT!
Obviously our medical teams don’t shoot their way into jobs; however, ensuring a scene is safe and secure before commencing patient care is essential. This is true on any mission, but you must be extra vigilant when responding to a GSW, stabbing, fire, explosion, building collapse, and the like. Check on scene safety en route to the job, if possible, and then confirm with the police or scene commander on arrival.
Don’t forget that scene safety is relative and dynamic: an assailant may return to the scene later, a distant fire may spread, secondary devices may have been placed to target responders. Keep your eyes and ears open.
TACTICAL EMERGENCY CASUALTY CARE (TECC) is the name of the game
Inspired by the military’s Tactical Combat Casualty Care (TCCC), TECC is an increasingly evidence-based, standardized approach for addressing preventable death in civilian trauma. Although geared towards the logistics and special needs of a tactical situation, the tenets apply to many of the scenes we encounter in prehospital medicine. At the core of TECC is a laser focus on what kills this patient population first, and how to treat it.
So your standard ABCs of ATLS/EMST fame become MARCH, ensuring massive hemorrhage is assessed and treated immediately. No sense putting that ET tube in if your patient bleeds out while you do the kit dump. This model of primary assessment also specifically calls out attention to head injury and the threat of hypothermia.
THINK ABOUT WHAT KIT YOU WILL NEED
With these priorities in mind, consider what kit you really need when responding to a high threat job, especially if a tactical situation is in progress (such as a standoff), or if there are multiple casualties (shooting, explosion). Do you really need two heavy trauma packs, a monitor, and an unwieldy stretcher as you enter a scene, or would you be better served to commandeer a cache of tourniquets, pressure bandages, hemostatic gauze, nasal/oral airways, and thoracostomy supplies? Keep in mind that many of these events are not static, and may require you to be mobile as the scene evolves.
BE AN EXPERT AT TOURNIQUET APPLICATION
During our practical workshops, it was clear that although we all understand how to use a tourniquet in theory, the actual mechanical application (particularly under stress, or with a patient on the ground) can be quite slow and fiddly. As any other kit we use infrequently in high stakes scenarios, we should become intimately familiar with the tourniquet and practice using it.
Two pro tips: 1) If you can’t immediately identify the source of major limb bleeding, place the tourniquet as proximal on the affected extremity as possible. 2) If bleeding continues despite your tourniquet, place a second one adjacent to the first.
Here’s a good overview video as a refresher.
CONSIDER OTHER POTENTIAL SOURCES OF INJURY
When evaluating a patient brought to you from a tactical scene, keep your mind that there are numerous ways someone can be injured: fragmentation (grenades, explosives), burns (flash bangs), chemical (pepper spray or hazmat), lacerations from broken glass, blunt trauma (restraint, impact weapons, falls), taser barbs, heat/cold illness, dehydration.
OUR JOB IS NOT TO KICK DOWN DOORS
Lastly, as mentioned during this CGD, nothing in our training or ongoing discussion of these tactical medicine issues prepares us to throw on body armor and go into the so-called “hot zone” with the police/tactical unit. This primary operational tactical medicine role is the responsibility of a dedicated group of specially trained SOT/SCAT paramedics who “provide medical support to Police tactical operations, in urban and remote settings, with specialist vehicles, uniforms and equipment available to ensure integration into high risk operations. Initial training on cover and concealment, tactical movement and awareness of tactical considerations is covered, with ongoing interagency training.”
THAT SAID: BE USEFUL
Much like the Ingleburn shooting, we may be on a scene with nothing medically happening for hours (if at all). Try to be as useful as possible. Start making sure the command structure knows there is a doctor-paramedic team on scene. Begin pre-planning your casualty collection point, how you will get additional supplies, where patients will be transported and how (easy when in MTC-rich Sydney, much harder in a bush town). Make sure everyone is drinking water. Help create shelters from the heat or cold. Be available to support the SOT/SCAT tactical paramedics, and provide advice and care for minor medical issues.
Sometimes the best thing you can do for the success of a prolonged mission is to just get people to wash their hands before eating.
To fill this educational void, you should have a listen to the recent prehospital podcasts that our very own Cliff Reid, Geoff Healy, and Karel Habig put out. They are available on iTunes under “Greater Sydney Area HEMS” or at the blog links below. There are a remarkable number of clinical/logistical pearls, as well as some new words to add to your lexicon.
(Thanks again to Dr. Clare Hayes-Bradley for presenting the latest Airway Registry and penning the subsequent discussion points below.)
To RSI or not to RSI, that is the question…
It’s foul weather, near zero degrees and torrential rain, it’s night, and you’re on a residential street 15 minutes away from the regional trauma centre by road. Your obese patient is unconscious with airway obstruction along with other signs of serious injury. To RSI or not to RSI? What factors might influence your decision making?
In favour of RSI in the vehicle would be the weather and a lack of nearby shelter (like a car port or service station). In favour of RSI at the hospital might be adequacy of basic airway manoeuvres & ventilation and short travel time. Your assessment of current airway patency and ventilation, together with your assessment of difficulty of intubation and patient positioning inside the vehicle may be factors (like can you physically adjust the stretcher head-up and place occipital padding). There may be other pressing clinical concerns that require urgent hospital intervention.
Our GSA-HEMS PHEA manual 2016 gives some suggestions on the pros and cons for on-scene versus hospital RSI.
Performing an RSI in a vehicle will feel different to an RSI at the back of the road vehicle with 360 degree patient access. Why not practice an ‘in-car’ RSI for your next RSI currency or sim?
My bougie is too rigid…..
Borrowed from prehospitalmed.com, with permission
So you can see the cords but that bougie just won’t go where you want it to – what are your options?
Consider optimal bougie ‘top control’ by your assistant
Consider your bougie grip – for example, some practitioners report the ‘Shaka’ or ‘kiwi’ grips can improve bougie tip control
Take the bougie out of the mouth to re-shape
Use our other bougie (hollow blue or solid white)
Intubate the trachea without adjuncts if able
Use a stylet as an alternative adjunct
Another thing to consider practicing at your next RSI currency…
Patients can appear agitated pre-RSI for many reasons including pain, fear, their pathology/injuries, or drug effects. In some cases IV or IO access for pharmacological control is impossible to achieve initially. Safe physical restraint of the patient to allow intramuscular sedation may be necessary. Needlestick injuries must be in everyone’s mind here and ‘safe sharps’ are paramount. Coordinating the sedation attempt with colleagues with clear language and explanation is important, as is being aware of your location and availability of resuscitation equipment if the response to the sedation is profound.
So what drug or dose would you choose in an adult male patient whom you suspect is agitated from severe pain. Consensus would suggest 2-4mg/kg IM Ketamine could be reasonably expected to produce the desired result – a patient calm enough to accept IV/IO access and further treatment.
Sydney HEMS acknowledges the Australian Aboriginal and Torres Strait Islander peoples as the first inhabitants of the nation and the traditional custodians of the lands where we live, learn and work.






 weather and a lack of nearby shelter (like a car port or service station). In favour of RSI at the hospital might be adequacy of basic airway manoeuvres & ventilation and short travel time. Your assessment of current airway patency and ventilation, together with your assessment of difficulty of intubation and patient positioning inside the vehicle may be factors (like can you physically adjust the stretcher head-up and place occipital padding). There may be other pressing clinical concerns that require urgent hospital intervention.
weather and a lack of nearby shelter (like a car port or service station). In favour of RSI at the hospital might be adequacy of basic airway manoeuvres & ventilation and short travel time. Your assessment of current airway patency and ventilation, together with your assessment of difficulty of intubation and patient positioning inside the vehicle may be factors (like can you physically adjust the stretcher head-up and place occipital padding). There may be other pressing clinical concerns that require urgent hospital intervention.


