

Here is a link to the paper that will be discussed at Journal Club

The following learning points are collated from Regional and Rural hospitals of NSW, Australia, represented here by a single fictional institution – Umbara Base Hospital. Cases are amalgamated and anonymised (including alteration of patient demographics) such that similarity to real patients is coincidental.
Below are some high-yield learning points collated from the Umbara Hospital trauma case review meeting.
Patients with blunt trauma with significant orthopaedic injury may have other significant other injuries that are difficult to assess on history and examination and easy to miss.
Here’s a good article on this.
Anchoring bias may also occur, particularly in inter-hospital transfers. These are higher risk patients for missed/delayed diagnosis. Reassess the patient from the start.
Elderly patients (>65) who sustain blunt chest trauma with rib fractures have twice the mortality and thoracic morbidity of younger patients with similar injuries. For each additional rib fracture in the elderly, mortality increases by 19% and the risk of pneumonia by 27%.
CXR is inaccurate in diagnosing the presence and number of rib fractures – hence we should have a low threshold for CT to further assess. Current best practice is the ChIP protocol.
Angioembolisation in renal trauma is effective in selected patients.
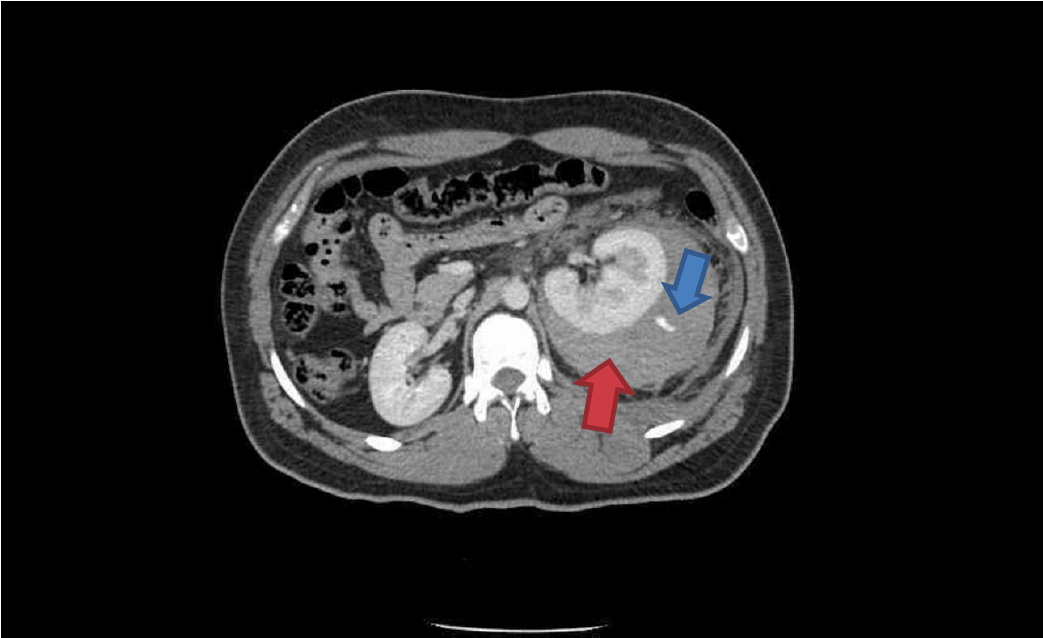
Trauma CT: Blue arrow is contrast ‘blush’=active bleeding point. Red arrow is perinephric haematoma.

Angioembolisation. Red arrow=coils in arcuate artery of kidney which has stopped the bleeding.
When transferring these patients from smaller hospitals to larger centres, consider whether initial destination should be the ED for rapid re-assessment prior to entering IR suite.
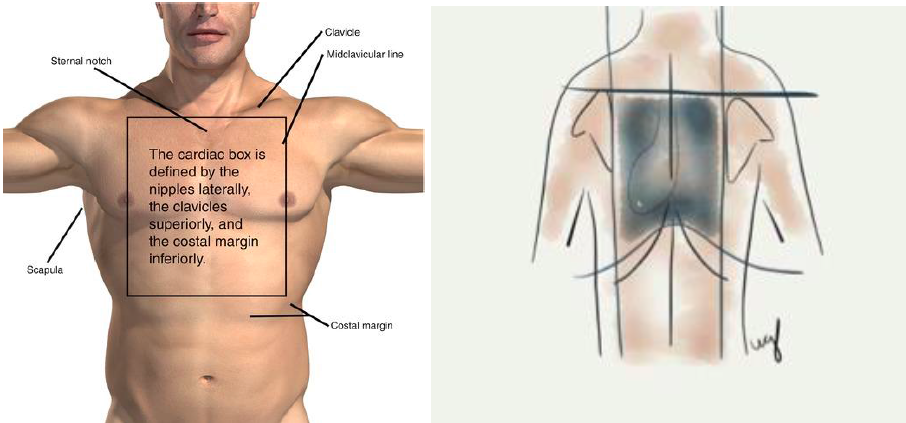
Anterior and posterior ‘cardiac box’
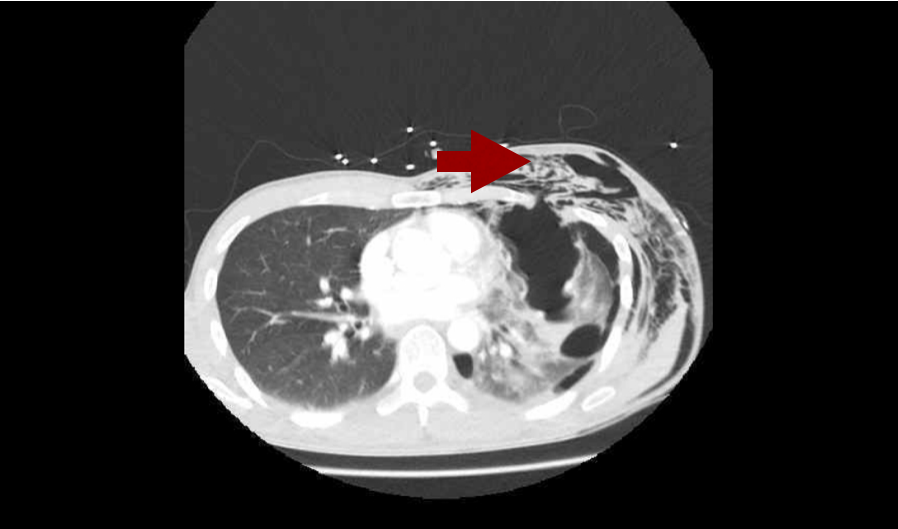
Penetrating trauma to the ‘cardiac box’ may result in cardiac injury and pericardial effusion leading to tamponade. A permissive hypotension strategy is followed where practical.
Diagnosis may be made by eFAST, bedside formal echo or by CT depending on clinical stability.
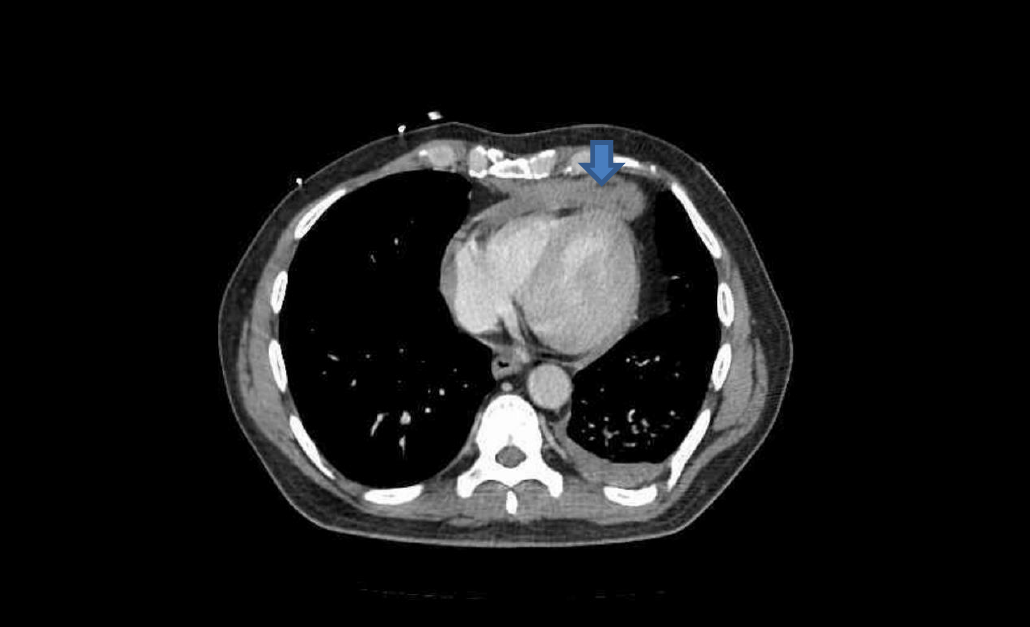
Axial CT showing anterior pericardial effusion (blood) from trauma (blue arrow)
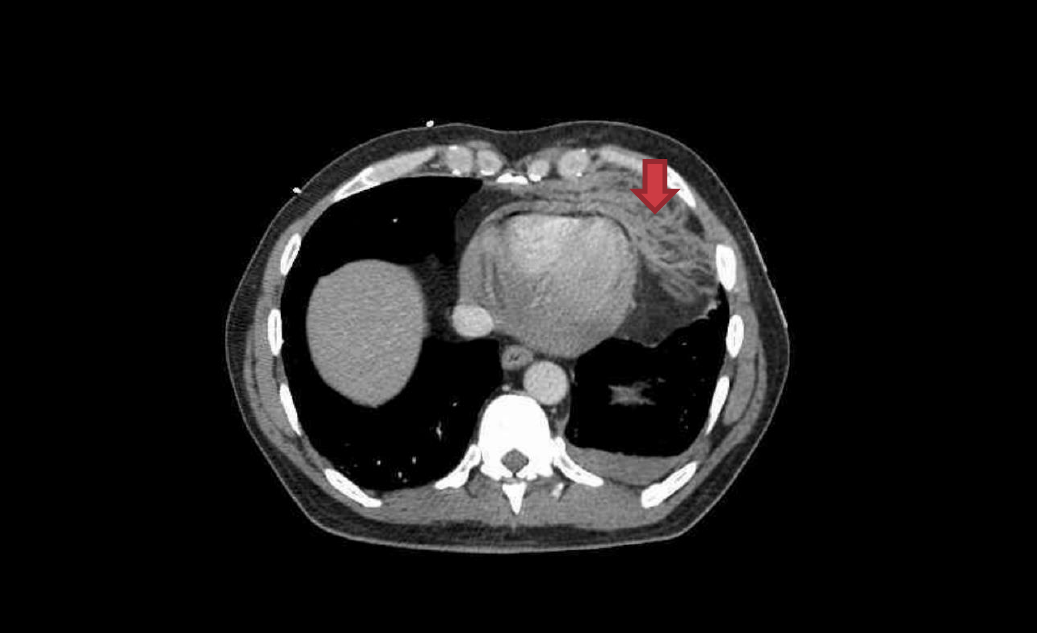
Pericardial fat stranding caused by pericardial blood (red arrow)
The key operative finding at the tertiary trauma centre was right ventricle laceration, which was successfully repaired.
The following learning points are collated from Regional and Rural hospitals of NSW, Australia, represented here by a single fictional institution – Umbara Base Hospital. Cases are amalgamated and anonymised (including alteration of patient demographics) such that similarity to real patients is coincidental.
Below are some high-yield learning points collated from the Umbara Hospital trauma case review meeting.
Always check the chest drain with a CXR – particularly check for the drain’s position and for complications such as kinking, as can be seen in this left sided CXR.

Pneumothorax is often associated with subcutaneous emphysema (free air in the tissues under the skin). It feels like bubble-wrap and looks like this on CT. Don’t press too hard though – it’s likely there are rib fractures underlying the air and they are extremely painful!
Trauma in older patients is increasing with our ageing population here in Umbara – ever improving management of chronic health conditions means people are living longer. It is difficult to predict mortality in elderly trauma and hence some scoring systems exist.
Geriatric Trauma Outcome: Age + (2.5x ISS) + 22 (if PRBCs administered)
Mortality: 205=75%, 233=90%, %, 252= 95%, 310=99%.
These scoring systems may help guide discussions with patients and their families in the future.
Data from the UK Trauma Audit and Research Network (TARN) showed that 2.5% of children in their database had suspected child abuse underlying their injuries. 97.7% of these children were aged <5yrs; 76.3% were aged <1yr. Injury severity score (ISS) was also greater in patients with suspected child abuse: they were 1.7x as likely to have an ISS score >15.
You can read more in this free-to-access paper.
IDENTIFY risk factors through history, examination, observation.
LISTEN and watch parent-child interaction
CONSIDER the possibility
DON’T DISMISS non-accidental injury as a possibility due to lack of physical findings
DOCUMENT carefully, clearly and contemporaneously
PREVENT by linking with services
KNOW your legal requirements for reporting
Although non-accidental injury can occur in the absence of these factors, there are several factors which have associations with non-accidental injury.
In the child:
Parent/Family:
Other concerning features:
Clinical/Attendance features:
Child Protection Courses: http://www.heti.nsw.gov.au/Courses/Child-Protection/
Non-accidental injury blog & podcast: http://stemlynsblog.org/child-protection/
When Umbara Base Hospital’s own Dr Tallie fell from her horse earlier this month and ended up being treated in her own Emergency Department, she was in a unique position in being able to provide constructive feedback around her own care with a full understanding of the processes of the hospital.
This month we invited her to share her thoughts at the trauma case review meeting and were delighted to learn the following.
Huge thanks to Dr Tallie for her insights – we wish her well on her recovery.
 Drs Natalie May, Geoff Healy, and Cliff Reid discuss missions in which the prehospital medical team is diverted to a hospital because their patient has been moved from scene to a (non-major) hospital.
Drs Natalie May, Geoff Healy, and Cliff Reid discuss missions in which the prehospital medical team is diverted to a hospital because their patient has been moved from scene to a (non-major) hospital.
While one might expect these missions to be easier from the point of view of having the hospital environment and resources to hand, they can in fact be more complicated and take longer than typical prehospital (primary) and interhospital (secondary) missions.
There are a number of reasons for this:
Nat, Geoff and Cliff discuss these challenges and how to tackle them, including how to introduce yourself, what language to use, how to integrate yourself into the team and offer support and if necessary leadership, the importance of a collaborative approach, and the critical contribution of the RT paramedic in making all this happen smoothly.
Resources referred to in the podcast
Prehospital Advanced Non-Technical Skills Handout (PANTS) Handout
Graded Assertiveness in the TeamSTEPPS® program
101 Reflective Lessons from a Year with Sydney HEMS

This second post from the Sydney HEMS ECMO education days summarises a great session by Retrieval Doctor and all-round legend Natalie Kruit on Troubleshooting in ECMO Retrieval.
As mentioned in Part One, the retrieval doctor is essentially there to look after the patient as a whole, while the separate ECMO team will oversee the function of the ECMO pump.
The first thing to know as a retrieval doctor is that the pump is primed with crystalloid – there is approx. 1L in circuit in total – so we should expect patients to be a bit unstable after transition onto pump!
There is an access line in or near vena cava – this draws blood into the pump. This is the negative pressure part of the circuit.
Blood drains into centrifugal pump, is oxygenated and is returned to the right atrium.
The Murray score is used for this: for a score >3 – consider referral to ECMO centre

Murray score: VV ECMO inclusion criteria
Pathologies that will do well: asthma, ARDS. The longer they’ve been on a ventilator, the less likely they are to do well on ECMO.
This occurs when the vein the cannula is sitting in is collapsing around the cannula.
Causes: hypovolaemia, anything altering venous return (eg coughing, sedation bolus, increased abdominal pressures)
Treatments: drop the revs, give volume, remove obstruction, consider and exclude tamponade
Once on VV ECMO – target lung protective ventilation: rest the lungs, minimise alveolar strain
Reduce FiO2 (target around 0.6 if possible: O2 toxicity, diffusion atelectasis from reabsorption), reduce the RR, increase PEEP (prevent alveolar closing and opening – maintain alveolar opening), smaller TVs (4mls/kg or even lower) (letting the ECMO circuit do the oxygenation)
Caused by
Targets: Platelets >50, Fibrinogen >1.0, INR <2.0, APTT 1.5x normal
If bleeding: TXA, FFP, platelets (prepare to do an ECMO circuit change as may clot) – don’t give protamine (you will get clots and that is maximum badness!
When SpO2 increasing on ECMO machine, the patient becoming hypoxic – this suggests recirculation (blood not getting to the patient)
Shunting on VV ECMO
The circuit may not be able to capture full cardiac output, so some deoxygenated blood is circulating. Preferentially this seems to go to the brain and heart. This can happen in someone whose circulation is hyperdynamic (eg sepsis, morbid obesity). The drainage cannula is a good determinant of flow (a bigger drainage cannula gives better flows).
Cardiac output >ECMO flow (if you set flow at 5L/min and the patient is hyperdynamic at 10L/min, only half blood vol will be going through circuit and being oxygenated)
Treatment:
This occurs when the access line and drainage line are sitting too close together so the flow is bypassing patient altogether! Or if there is increased intrathoracic/intracardiac pressure (e.g. tamponade)
You may see a low arterial SaO2 and high access cannula SaO2.
Treatment:
There are two different cannulation options for VA ECMO.
You’ll get some mixing of the deoxygenated blood from the ventricle with the oxygenated blood from the ECMO circuit – the more contractile the ventricle, the more distal the mixing point. There’s a nice interactive critical care case here that covers some of this.
If the lungs are not working and the heart is starting to recover and therefore has some recovering ejection fraction, the heart will preferentially eject to coronary and cerebral circulations (so check the ECG for signs of cardiac ischaemia) – it’s also helpful to have a SpO2 probe on right hand to see differential hypoxia early.
In this scenario the heart is pumping (so there is a native cardiac output) and that is picking up and distributing deoxygenated blood that we can’t capture with ECMO flow. You may see demarcation of skin tone change across the trunk and/or the ECG may show ischaemic changes. There’s a nice diagram here which comes from this open access paper in Circulation (clicking the link will download the PDF).
Treatment:
When severe end organ damage has occurred (e.g. AST/ALT very high, lactate >10 and not clearing) we have missed the boat!
We are aspiring to the least damaging lung ventilation
Causes:
You shouldn’t need to give a fluid bolus – so if doing this, consider LV failure is evolving (dilating LV with inability to pump out)
Offloading the LV – may need to decompress by creating a vent between L and circuit, R heart – there’s potential to use impella to suck blood out directly
If you work for Sydney HEMS, take a look at the new ECMO class available through the virtual learning environment.
A/Prof Forrest talked a little bit about VA ECMO in sepsis.
The key to the septic shock definition is MAP 60mmHg (or inotropes required to keep it here).
Most adults dying from sepsis do so in a high output state (increased cardiac output with decreased systemic vascular resistance): this paper from 1984 looked at 20 patients with severe septic shock – 50% had moderate to severe decrease in left ventricular function. Notably they found the left ventricular ejection fraction had returned to normal within ten days in those who survived.
This leads us to consider whether low ejection fraction might be a good thing in patients with septic shock – this review by Vieillard-Baron et al from 2001 seems to support the hypothesis.
It’s possible, then, that the relationship between survival and non-survival depends on systemic vascular resistance in the context of vasoplegia – this allows for left ventricular ejection fraction to be maintained against lower resistance
There’s some evidence we might consider in paediatric patients:
MacLaren et al described their experiences with VA ECMO for septic shock in children.
They looked at 45 patients, of whom 21 survival (47%). In terms of central vs peripheral VA ECMO, survival proportions were 73% vs 44% and no survivors severely disabled. The authors felt that their data suggested that central configuration might provide a survival advantage.
The same team published a further paper in 2011: in this paper they studied 23 patients, 17 of whom survived to discharge (74%): they noted that a high lactate predicted worse survival.
As a result of this work, the American College of Critical Care Medicine’s paediatric sepsis guidelines published in 2017 include ECMO if the child has persistent catecholamine refractory shock.
For adults the data is lacking; literature only describes around 200 adults on VA ECMO when case series are combined and there are considerable different baseline characteristics between patient groups.
Cheng et al studied adult patients requiring ECMO for the management of sepsis in their paper on predictors of survival: they found that gram +ve sepsis does better than gram –ve or fungal.
There is also the possibility (in adult patients) of using V-AV ECMO: this is when a second return line is sited in the internal jugular (or similar) with the aim of providing oxygenated blood to the right heart. The femoral artery is part of a higher pressure circuit than the internal jugular line and it can be tricky to regulate flow between the two lines. As yet there is little data on this: this case series by Yeo published in Critical Care in 2016 reports a 50% survival with this technique for adults with severe ARDS and septic shock.
For paediatric patients – central VA ECMO seems the best option
For adult patients:
In summary, VA ECMO in septic shock seems to be good for:
but more evidence is needed.
Loads of resources over at IntensiveCareNetwork.com
ECMO literature summaries – Life in the Fast Lane

Most of the following post is taken from the recent Sydney HEMS ECMO Education day with some taken from an earlier ECMO education day and amalgamated into a huge amount of notes.
Associate Professor Paul Forrest, a Cardiothoracic Anaesthetist and ECMO Specialist from RPA Hospital kicked off the day with an overview of the evolution and current state of ECMO services in NSW. He has a full uploaded presentation here you might be interested in or you can watch the full video below.
There are agreed statewide indications for ECMO – clicking on the link will take you to the document.
Patients are routed to St Vincent or RPA as per the Medical Retrieval Unit who oversees the mission.
The initial service commenced prior to the H1N1 outbreak – this paper in JAMA Oct 12 2009 describes how the service was utilised during the outbreak. 68 patients were treated with ECMO for a median of 10 days (IQR 7-15 days) with 48 surviving to ICU discharge (32 to hospital discharge, 16 still inpatients) at the time of publication.
The Cardiohelp pump is used with a customised footplate. When an ECMO team is tasked for a retrieval mission, the team will come with four custom packed retrieval packs of their own.
58% of ECMO transfers are transported by road, 27% by fixed wing and 15% by helicopter.
Feb 2016 figures: 68% survival to discharge overall, 72% in resp subgroup and 60% for cardiac subgroup
The St Vincent’s team, headed up by the wonderful Sean Scott, joined us for an ECMO themed sim. Learning was centred around an interactive simulation, the retrieval of a 55 year old patient from a smaller hospital in conjunction with the ECMO team.
Our role in these missions as the retrieval team: to take care of the patient, while the ECMO team takes care of the ECMO machine and pipes (“it’s not about the plumbing”). The full talk is shown in the video below.
ECMO is basically a heart and a lung – a pump and an oxygenator. Where you plug in the pipes determines the sort of support you (the patient) get(s).
VV – oxygenation, no cardiovascular support
VA – also generates a blood pressure, essentially a cardiopulmonary bypass machine
We should consider ECMO as a bridge; generally it is used as a bridge to recovery but sometimes to a decision (further resuscitation? Transplant?) or definitive intervention (treatment of cause of cardiac arrest).
This is effectively lung bypass, used when the “lungs don’t work” – there are many causes, for example:
Needs to be a potentially reversible cause
This is effectively heart and lung bypass, used for support in circulatory failure – cardiogenic shock is the most common/obvious reason (although the underlying cause may be MI, overdose etc.)
Trauma? – has been used in hypotensive trauma patients
Sepsis? – jury is out on whether this is a good idea (how reversible are the processes involved?)!
Most common is femoral/femoral VV cannulation
Fem/fem – two cannulae in IVC, one draining and one returning – can’t use two multistage cannulae (recirculation – when blood doesn’t actually flow through the circulation – is very high)
Fem/jug placement avoids this
Now features in the 2015 ALS guidelines under “consider” (extracorporeal CPR)
2CHEER (the study into LUCAS plus ECMO for out-of-hospital VF arrest) is ongoing in Sydney
However, it doesn’t “consider” all the logistical work involved in getting people onto ECPR
ECPR means we should add a few new links to the chain of survival – mechanical CPR on scene, ECMO in ED, straight to cath lab
Common patient scenario – refractory VF, PEA or asystole but after ECMO perfuses the coronaries, ROSC may occur quickly.
ECMO remains on after ROSC (the flow may be dropped a little) – the patient is usually in cardiogenic shock so needs the ongoing support.
Pit crew concept – everyone has defined roles, printed on role cards which they wear
This video shows how this is trained for through simulation.
LUCAS is used as a bridge to ECMO, ECMO is used as a bridge to intervention.
The target of ECPR is maintenance of cerebral perfusion while reversible causes are addressed.
Prehospital Training for 2CHEER was key, with a strong focus on changing the dynamics of arrest calls.
Put LUCAS on early, decision for eligibility early, transport early (with definitive airway if possible)
BatPhone activation to the ECMO centre is essential for team preparation
Clear role development and allocation with role cards (A5)
This training is not particularly frequent – one a month or so – which is helpful for refreshing and framing behaviour.
No! There are STOP criteria – although in practical terms it is advised that processes continue until there is a reason to stop
Transoesophageal Echo is used to guide cannula placement
There is a strict 90mins cutoff – if the patient has not been (ECMO) cannulated by 90mins from arrest time, efforts should stop (in reality this means the patients need to arrive in ED at 60mins from arrest time). No cases in the Sydney registry have not achieved this as yet!
5,000 units of heparin are given when the cannnulae go in. An extra (approx.) 7,000 units are given with the pump (which is primed with 10,000 units, there is some loss during connection).
The venous line is connected first due to risk of clots – they would then be sucked into unit, not into brain (as would occur if arterial line placed first).
VF arrests can occur with SAH – 15-20% of patients on ECMO end up with ICH (pre or resultant), CT brain is deferred until after definitive cardiac intervention, which may be >24h.
The team aims to get the patient onto ECMO on then thrombolyse – there is a potential for catheter directed lysis. Half dose used thrombolysis has been used as per MOPETT until now but radiology support for catheter directed is now available.
In-hospital, the team might be more lenient with rhythm (but would still need to know there’s a reversible cause)
Usually complications occurring immediately are related to cannulation – bleeding, haematoma, kinked wires, femoral nerve damage, arterial injury.
In standard elective VA ECMO, clinicians would put in a backflow cannula from arterial cannula to perfuse the distal limb. Smaller cannulae are used in ECPR to facilitate distal perfusion; after angiography, a backflow cannula is sited.
Longer term complications include: bleeding/clotting, infection plus the complications of a long ICU stay
(this is essentially a checklist for the ED Consultant)
Can stop LUCAS but priority is excellent ongoing CPR
Defibrillation is not necessary during the cannulation phase
Immediate term: difficulty getting access, wrong vessels (VV in arrest, AA), haematoma formation – surgical backup (for cutdown) and TOE confirmation can be helpful
Checklists are available and helpful e.g. suck down (insufficient volume to fill venous drainage cannula) – see more info in part two
It’s not awesome as yet – there are not many RCTs.
The paper by Kim et al in Resuscitation (2012) was a review comparing conventional care with ECMO – suggests better neurologically intact survival
(CPR, hypothermia, ECMO and early reperfusion)
This study took place in Melbourne (hypothermia was dropped) – there’s a great review of this paper over at The Bottom Line.
(Conventional ventilator support vs ECMO for Severe Adult Respiratory Failure)
This study looked at the benefits of referral to and treatment in an ECMO centre – the authors found a survival benefit with NNT 7
Notably although 90 were randomised to ECMO, only 70 went onto ECMO
You can find another great review over at the Bottom Line.
Loads of resources over at IntensiveCareNetwork.com
ECMO literature summaries – Life in the Fast Lane
The Physician Response Unit – An overview. Bill Leaning, Critical Care Paramedic, London Ambulance Service and London HEMS
We were privileged to hear from Bill Leaning via Skype, who spoke about the Physician Response Unit in London. Established nearly 20 years ago, it represents a productive collaboration between London’s Air Ambulance, Bart’s NHS trust and the London Ambulance Service. It’s vision of bringing the emergency department to patient’s homes is achieved by having senior emergency department doctors and paramedics travel by car to patients in the community. Community initiated treatment helps prevent unnecessary ED presentations and ambulance transfers. As well as the obvious benefit to the patient, the collegial relationship between the two clinicians gives each a valuable insight into the others role and skill set. The service has recently been remodeled to allow it to deliver community emergency care 24 hours a day, 7 days a week.

The Anatomy of a Difficult Case. Dr James Moran – Retrieval Registrar, Sydney HEMS
Jamie discussed the value of reflecting on difficult cases and bravely used one of his own recent cases to illustrate the point. Indeed, the Australian Medical Council’s Code of Conduct recommends that “Maintaining and developing knowledge, skills and professional behavior……. requires self-reflection”. Although there is little guidance available on how to actually do this, there is no doubt that the ability to critically reflect on one’s performance and ask hard questions of yourself will inform your future practice for the better. Suggestions include keeping a reflective logbook, and formal peer review.
An update from the Institute of Trauma and Injury Management. Michael Dinh – NSW ITIM
The NSW Institute of Trauma and Injury Management (ITIM), an institute within the Agency for Clinical Innovation (ACI), is the body responsible for overseeing, coordinating and supporting the NSW trauma system. Clincial director, Dr Michael Dinh, spoke about the role of ITIM in influencing access, care, outcomes, education, research and quality of trauma care in the NSW region.

Don’t forget there will be no Clinical Governance Day on the 27th December. The next meeting on the 13th December will be a combined Education Day and Clincial Governance Day. See you then.



