

The following learning points are collated from Regional and Rural hospitals of NSW, Australia, represented here by a single fictional institution – Umbara Base Hospital. Cases are amalgamated and anonymised (including alteration of patient demographics) such that similarity to real patients is coincidental.
Below are some high-yield learning points collated from the Umbara Hospital trauma case review meeting.
Chest drains
Always check the chest drain with a CXR – particularly check for the drain’s position and for complications such as kinking, as can be seen in this left sided CXR.

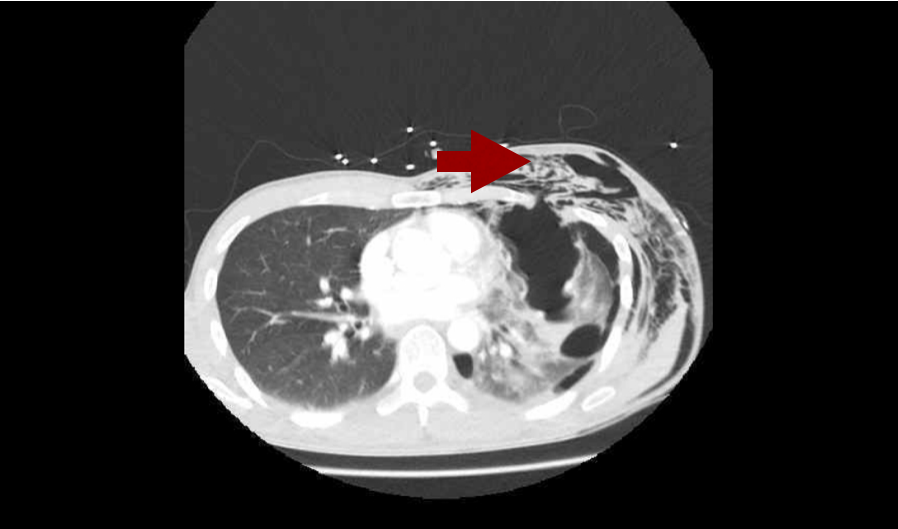
Pneumothorax is often associated with subcutaneous emphysema (free air in the tissues under the skin). It feels like bubble-wrap and looks like this on CT. Don’t press too hard though – it’s likely there are rib fractures underlying the air and they are extremely painful!
Elderly trauma
Trauma in older patients is increasing with our ageing population here in Umbara – ever improving management of chronic health conditions means people are living longer. It is difficult to predict mortality in elderly trauma and hence some scoring systems exist.
Geriatric Trauma Outcome: Age + (2.5x ISS) + 22 (if PRBCs administered)
Mortality: 205=75%, 233=90%, %, 252= 95%, 310=99%.
These scoring systems may help guide discussions with patients and their families in the future.
Non-accidental Injury in Children
Data from the UK Trauma Audit and Research Network (TARN) showed that 2.5% of children in their database had suspected child abuse underlying their injuries. 97.7% of these children were aged <5yrs; 76.3% were aged <1yr. Injury severity score (ISS) was also greater in patients with suspected child abuse: they were 1.7x as likely to have an ISS score >15.
You can read more in this free-to-access paper.
What can we do?
IDENTIFY risk factors through history, examination, observation.
LISTEN and watch parent-child interaction
CONSIDER the possibility
DON’T DISMISS non-accidental injury as a possibility due to lack of physical findings
DOCUMENT carefully, clearly and contemporaneously
PREVENT by linking with services
KNOW your legal requirements for reporting
Risk Factors for NAI
Although non-accidental injury can occur in the absence of these factors, there are several factors which have associations with non-accidental injury.
In the child:
- Chronic illness, disability or developmental problem
- Prematurity
- Age of child
- “Difficult” behaviour
Parent/Family:
- Unwanted pregnancy
- Young parents
- Single parent family
- Relationship problems
- Exposure to drug and alcohol abuse and/or family violence
- Low socioeconomic status
- Social isolation
- Physical or mental illness in a parent
Other concerning features:
- Poor hygiene
- Dirty clothes
- Missing a lot of school
- Previous contact with FACS / CPU
Clinical/Attendance features:
- Delay in presentation
- Injury not explained by story
- Inconsistent with developmental ability (know developmental milestones! Here’s a quick reminder)
- Inconsistencies in history and changes over time
- Unexplained or unwitnessed fall with neglect
- Previous suspicious injuries
- Unusual parent – child interaction
- Failure To Thrive (FTT)
- Resuscitation efforts caused injuries
- Patterned bruise/burns; certain distribution
- Spiral/transverse long bone fractures, particularly in non-mobile children
Child Protection Courses: http://www.heti.nsw.gov.au/Courses/Child-Protection/
Non-accidental injury blog & podcast: http://stemlynsblog.org/child-protection/
From the Horse’s Mouth
When Umbara Base Hospital’s own Dr Tallie fell from her horse earlier this month and ended up being treated in her own Emergency Department, she was in a unique position in being able to provide constructive feedback around her own care with a full understanding of the processes of the hospital.
This month we invited her to share her thoughts at the trauma case review meeting and were delighted to learn the following.
- Prehospital methoxyflurane is an excellent analgesic and she was very grateful for it
- She found the experience had increased her trust: she was happy to put her life in hands of the staff of Umbara Base Hospital and has a renewed appreciation for them all as a result
- She particularly noted that nurses are awesome (both during her ED and ICU stays): she added, “it’s the ‘little things’ that make all the difference”.
- Having experienced both, she found regional block much better in the pain management of her rib fractures than drugs.
- Overall she was dismayed to realise just how long bones take to heal.
Huge thanks to Dr Tallie for her insights – we wish her well on her recovery.

