Sydney HEMS were fortunate to have a Dr. Dan Adams, Director of the Central Australian Retrieval Service, present on his experience in the Red Centre.
The Central Australian Retrieval Service, based in Alice Springs, certainly has some differences from our Sydney based HEMS services. The patients, pathology and environment pose some unique challenges to our central Australian colleagues, we were glued to our seats hearing how you brought the highest level of care to these remote and demanding clinical situations. Dan guides us through the design of their service, and the logistics of serving a catchment with a diameter over 1200km, covering over a million square kilometers!
Thank you Dan for sharing your experiences and expertise!
At Greater Sydney Area HEMS, we carry a hyper-angulated (D-blade) option for our C-MAC video laryngoscope, but in our inter-hospital equipment bag. This means that it is not necessarily immediately to hand for pre-hospital missions (in part to avoid accidental mix-ups with the primary intubation kit), although can be utilised with some forethought if required.
Greater Sydney Area HEMS does not currently utilise or support the ‘universal’ use of hyper-acute video laryngoscopy (HAVL). From an organisational point of view, it can be healthy to question the status quo and explore alternative ways of working. We were therefore thrilled that Dr Nicholas Chrimes joined us at a recent Education Day to deliver an excellent HAVL workshop and interactive talk. Dr Chrimes is a Consultant Anaesthetist in Melbourne who wears multiple hats, including being a co-founder of the Safe Airway Society, and creator of the Vortex Approach to airway management. We particularly applaud his enthusiasm to engage with a group of arguable sceptics!
Below you can find a recording of the interactive talk, highlights from the workshop, and related resources.
Welcome back to the Sydney HEMS debrief. We are up to episode 11!
Today, we are pivoting towards toxicology. Specifically, we discuss some of the more common toxidromes encountered pre-hospitally, how they cause cardiac arrest, and what providers – in particular pre-hospital providers – may do in order to best resuscitate these patients.
In addition to some broader and very applicable learning themes pertinent to any toxidrome, we discuss
Beta-blockers
Calcium channel blockers
Amitriptyline
Quetiapine
…and more
Of course we are not doing discussing this alone. We are so luck to be joined today by a clinical toxicologist, Dr Úna.
Dr Úna Nic Ionmhain graduated from Trinity College Dublin, and subsequently trained in Emergency Medicine in Perth. She completed a Pre Hospital and Retrieval Medicine year with CareFlight NSW as well as a poisons fellowship. She is now a staff specialist FACEM at Liverpool Hospital NSW, and a clinical toxicologist with the NSW Poisons Information Centre. She has an academic interest in HIET in toxicology for cardiogenic shock, which was the focus of her masters thesis, and is a passionate educator with a particular interest in cardiotoxicity.
We sure hope you enjoy this episode, and until next time, we hope you have a great week.
It’s 1am at a motor vehicle accident. RSI is complete; the patient is being loaded to the ambulance and established on the Hamilton ventilator. What rates should we start the sedative infusions at? And with everything else going on, how do we quickly individualise this between a 60 kg patient with internal bleeding and a 90 kg patient with burns?
A busy night shift, it’s now 3am and we’re with a septic patient who urgently needs transfer for source control. The isolated referring hospital has done an excellent job, but the patient is no longer fluid-responsive and the metaraminol infusion isn’t cutting the mustard. We want to start peripheral noradrenaline—what rate should we use, and when should we consider adding agents like adrenaline or vasopressin?
The next night, we’re on a fixed-wing transfer with an awake subarachnoid haemorrhage patient who’s becoming progressively more hypertensive. There’s no mobile signal, but we should know how to prepare and start a labetalol infusion… what’s the dose again? It’s been a while.
We are only human. Sometimes it’s about knowing where to find the right information fast rather than trying to hold it all in memory. We should also aspire to individualised care for our pre-hospital and inter-hospital patients, not a one-size-fits-all approach. We already accept this in paediatrics, where the beloved paediatric drugs aide-mémoire is never far away. For the same reasons, we’ve developed a concise adult drug infusions aide-mémoire to support informed, tailored decisions—especially when cognitive bandwidth is tight.
The aide-mémoire is designed to be printed at A5, laminated, and it fits snugly inside the front pouch of our current drug thigh-pouch. Of course, an electronic copy can also be saved offline to your device—but consider how handy that will be at a genuinely time-critical moment.
We’d be very grateful for Greater Sydney Area HEMS staff feedback on the utility of this aide-mémoire—what helps, what doesn’t, and constructive suggestions. We’re keen to keep it concise and easy to use in urgent situations. Please provide feedback via the QR code on the printed card or by clicking this link: https://tinyurl.com/adultiviaidememoire
Disclaimer:This aide-mémoire is designed to support, not replace, clinical judgement. It does not constitute a protocol. Final decisions, including drug choice, dosing and monitoring, remain the responsibility of the treating clinicians, who must consider the individual patient, context and local guidelines. As always, our posts do not constitute clinical advice,
Ventilating a severe asthmatic can be a humbling experience. Even though its principles are often discussed, there are nuances to avoiding dynamic hyperinflation that often leave us wondering if we’ve done everything possible to safely ventilate the patient in front of us.
Two Quick Concepts Before We Get Started- The Equation of Motion and Large Vs Small Airway Flow Waveforms
The Equation of Motion represents the components that contribute to Total Airway Pressure. These components can be broken down into:
Resistive Airway Pressures– This is the pressure generated when gas flows through the conductive airways. This pressure is the product of Resistance x Flow. It’s worth remembering that flow represents Volume/Time. This explains why your airway pressures will be high not only during bronchospasm, but also when high tidal volumes are applied over short inspiratory times. Given this pressure is flow dependent, during breath holds (where flow is 0) this pressure does not contribute to the measured Airway Pressure. Because this is not a pressure applied to the alveoli, this pressure does not risk injury to lung parenchyma. An inspiratory pause on the ventilator will therefore remove this pressure from the peak inspiratory pressure the difference between the two will give us a good idea as to the degree of resistance present.
Alveolar Pressures– Alveolar Pressure is independent of flow and is able to injure lung parenchyma. The higher the volume applied, and the worse the compliance, the higher the alveolar pressure will be. However, this pressure is on top of the PEEP we provide and the intrinsic PEEP generated during gas trapping. Therefore, alveolar pressure= Tidal Volume/Compliance + PEEP + PEEPi. It’s worth noting that even though asthma is a disease of airway resistance, a gradually climbing PEEPi will lead to higher alveolar pressures and barotrauma. This gradually climbing alveolar pressure will also push the compliance curve to the right, towards the flat portion of the curve and therefore worsen the compliance which will also contribute to worsening compliance. This means that if serial inspiratory breath holds are showing a gradually rising pressures, it should raise alarm bells for gas trapping.
Putting this together, Airway Pressure= Resistance x (Volume/Time) + (Volume/Compliance) + PEEP + PEEPi
The second concept to touch on is the Expiratory Flow Waveform, and how this differs between small and large airway obstruction. The normal expiratory flow waveform is a triangular, shallow curve that returns to the baseline. Generally, >80% of the inspired volume (seen by the area under the curve of the inspiratory flow curve vs expiratory flow curve) should be expired in the first second.
Lower airway obstruction, as seen severe bronchospasm, represents heterogenous obstruction that worsens as lung volumes decrease. Therefore, a deep, concave curve develops with a baseline that does not return to zero. The failure to return to zero may be extremely subtle. Usually <80% of of the inspired volume will occur in the first second.
Large airway obstruction is an important differential. In this case, there is a fixed obstruction to expiratory flow and therefore, there is a near linear expiratory flow curve with <80% expiration in the first second and a failure to return to baseline. This is usually the result of biting on the ETT, sputum plugs or blood clots in the tube, or an expiratory valve on the ventilator that has gotten stuck. Start with a suction and check the ETT position, then potentially an X-ray and bronchoscopy and muscle relaxation. In the context of presumed asthma, an inhaled foreign body can cause high airway resistance, gas trapping and pneumomediastinum. A linear expiratory flow curve should prompt you to consider this in asthma.
Medical Management Options for Severe Asthma- What Else Can We Optimise?
Oxygen- Targeting a sats of 94-98% is reasonable, as higher FiO2s may lead to VQ mismatch
Beta-Agonists-Salbutamol needs to be nebuliser at 10-12L/min to generate the 1-3microm particles needed to reach the target airways. Less than 10% of nebulised salbutamol reaches the target. This is the argument for IV salbutamol, but it carries an increased risk of adverse side effects without any proven additional benefit. Consider your options for routes of administration. MDI via T piece is a simple quick way to administer salbutamol, but this job requires someone dedicated to ensuring every dose is received on schedule. Continuous nebulisers are an option, but accidentally tipping the nebuliser is something to be aware of. Even small ICUs frequently stock ultrasonic nebulisers, which theoretically can deliver smaller particles more distally. If you’re not convinced the inhalation route is delivering enough, consider changing to IV. Adrenaline offers a familiar IV alternative and covers you for anaphylaxis you’ve incidentally missed. IV adrenaline boluses are a good.
Anticholinergics- Meta analysis level evidence shows benefit when ipratropium is added to salbutamol in severe asthma, but the optimal dosing remains unknown. In high doses for intubated patients, remember anticholinergic housekeeping such as eye care and an IDC.
Steroids- Steroids carry a benefit in doses up to 800mg/day of hydrocortisone. It’s worth noting the concerns for necrotising myositis when combing high dose steroids and NMBA in severe asthma.
Magnesium Sulphate- Nature’s calcium channel blocker. A Cochrane Review demonstrated benefit in adults. Doses of 5-10mmol over 20min are safe but associated with hypotension and flushing. Keep track of when the next dose is due.
Aminophylline- A phosphodiesterase inhibitor with a narrow therapeutic index. A Cochrane Review failed to identify any population group where aminophylline was beneficial. Aminophylline has fallen out of favour in adult ICUs but in children, a loading dose of 10mg/kg over an hour can be administered.
Ketamine- Likely a modest bronchodilator via anticholinergic effects. Small RCTs have failed to show a benefit in acute severe asthma. It offers a good induction option and a continuous infusion is commonly used. Beware the associated bronchorrhea in patients with increased mucous production.
Volatile anaesthetics- You may encounter the AnaConDa device, a small volatile anaesthetic vaporiser and HME designed to fit into standard ventilators and decrease the amount of volatile needed to be delivered compared to a standard anaesthetic machine. The AnaConDa measures and displays the end-tidal% of the volatile rather than a MAC to target. Alternatively, a transporting these patients to theatres for sevoflurane or isoflurane may be a rescue option.
Muscle relaxation- now is not the time for ventilator dyssynchrony.
VV-ECMO- obviously this is a step beyond magnesium and ketamine, but status asthmaticus is a good indication for VV-ECMO. The pathology is reversible, the patients are often otherwise well and the ECMO run is likely to be short. These patients are unlikely to require high flows on ECMO as oxygenation is not generally their problem. Instead we’re using ECMO for the sweep’s decarboxylation. It’s worth thinking about this if you’re putting in central lines. Bilateral femoral vein access for VV-ECMO is likely to be required, but if you’re going to choose the RIJ, the pleura is likely to be sitting higher than expected due to hyperinflation, and the myocardium will be irritable from the beta-agonists, so a liberal guide wire may lead to arrhythmias. Ideally, ECMO should be started before barotrauma occurs given the high incidence of chest drain bleeding once cannulated.
If all else fails, disconnect the tube and manually compress the chest.
Deciding Who To Intubate?
Generally speaking, patients are going to be better at managing their ventilation than we are. Deciding to intubate them is a clinical decision based on the information available, but there are features that favour intubation over observation:
Altered mental status
Paradoxical respiration
Bradycardia (preterminal)
pH <7.2 or a falling pH and climbing PCO2 despite maximal treatment
History of previous intubation for asthma
Pulsus Paradoxus >25mmHg or a loss of Pulsus Paradoxus implying respiratory muscle fatigue (preterminal)
Factors that favour continuing trialing medical management before intubation include:
Minimal drug therapy to date
History of previous rapid improvement with steroids
A clear precipitant that has subsequently been removed
Time availability
Mechanical Ventilation in Severe Asthma:
The goals for ventilating an asthmatic are:
pH >7.2
Plateau Pressure <25
PEEPi <10-12
Everyone will draw their own line in the sand with these parameters. In difficult to ventilate asthmatics, a pH of >7.15 can be tolerated provided a PaCO2 is <90. Generally speaking though, permissive hypercapnia is the safest approach, provided the pH is safe. The patient groups where permissive hypercapnia is less of a good idea include pregnancy, TBI, pulmonary hypertension and severe right heart failure.
The importance of a plateau pressure <25 is often understated. Asthma isn’t a disease of compliance and therefore an elevated plateau pressure should be a warning of gas trapping. As described above, the plateau pressure is the pressure during no flow, and only represents alveolar pressure. If the alveolar pressure is increasing it implies that PEEPi is increasing, and that the compliance curve has been shifted to the flat portion due to dynamic hyperinflation. Even though we conventionally target a plateau pressure <30, in asthma a plateau pressure target <25 has been suggested to be more sensitive to DHI than measured auto-PEEP. A plateau pressure can be measured on the Hamilton. The other important differential for a rising plateau pressure in this context is a tension pneumothorax.
So what ventilator settings do I start with? Whatever you do, give plenty of time to exhale. My standard recipe is:
1. Volume control mode – This allows more accurate control of minute ventilation provided Pinsp alarms adjusted. A pressure control mode will lead to changing volumes delivered over time as the asthma improves or deteriorates. 2. FiO2 titrate to saturation 94-98% – Avoid oxygen toxicity, reabsorption atelectasis and VQ mismatch 3. PEEP 0? – Controversial, but ‘ZEEP’ avoids additional PEEP that may worsen airflow limitation. Another conventional approach is to set PEEP at 60-80% of PEEPi, to prevent overinflated alveoli collapsing surrounding airways and preventing their own emptying. – Remember, driving pressure will be Pplat-PEEPtot (target <15) 4. Target minute ventilation <115ml/kg/min (~8-10L/min) 5. Resp rate 8-12 6. Vt 6-8ml/kg 7. I:E ratio of 1:4 and no inspiratory pause. See what is needed to allow the expiratory flow waveform to return to 0 and adjust as needed. 8. Adjust alarms to avoid pressure limiting for high inspiratory pressures provided plateau pressure <25 (set Pinsp alarm as high as the ventilator will let you) Because this is a disease of airway resistance, high airway pressures with normal plateau pressures aren’t dangerous to the lung parenchyma. Beware, the Hamilton’s Pinsp alarm is 60, which means it pressure limits at 50. That’s not very high in the scheme of severe asthma. – Targeting Pplat <25 allows monitoring for DHI. – Pplat >25 should prompt immediate inspection for pneumothorax or over distension. 9. Wet circuit -If you’re going to be waiting in someone else’s ICU for a protracted period of time, removing the HME and going onto a wet circuit removes additional resistance from circuit.
What Additional Monitoring or Clinical Clues Are Helpful Once We’re Ventilating?
Chest wall movement- quick and simple. If the patient’s chest is moving more, we’re winning. If it’s moving less, we aren’t.
Lung ultrasound- severe obstructive airway disease can cause decreased lung sliding, but an important differential is a pneumothorax due to barotrauma. Subcutaneous emphysema may make this difficult.
End-Tidal CO2- the ‘shark fin’ is well described. Out of interest, days down the track when ICU is weaning to spontaneous ventilation, watch the ETCO2 waveform for ‘curare clefts’ that suggest that the patient is unable to effectively trigger the ventilator due to high PEEPi. The trigger is generally a flow below set PEEP, and the patient will now need to overcome PEEPi + PEEP to trigger the ventilator. A bobbing head at this time point is often a clue that either more PEEP is needed or it’s too early to wean muscle relaxation.
ABG- aim pH >7.2 with permissive hypercapnia. Expect a lactic acidosis, hypokalaemia and hyperglycaemia in the context of beta-agonists and steroids.
Arterial line trace- a worsening pulsus paradoxus is concerning, but in a spontaneous ventilating patient, a sudden loss of pulsus paradoxus should be a red flag for imminent arrest.
Inspiratory and Expiratory Pauses- Target your inspiratory pause pressure <25 and expiratory pause <10-12 to help detect gas trapping.
Expiratory Flow Curve- As discussed above, a deep concave curve implies bronchospasm, whereas a straight linear curve implies an alternative diagnosis. Assessing whether a bronchospastic expiratory flow curve returns to zero can be very subtle, as they may be nearly asymptotic. If it’s that small, does it really matter? Well, if every breath traps an additional 5ml at a respiratory rate of 10, by 60 minutes, 3 litres will have been trapped. It doesn’t take much.
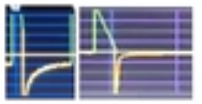
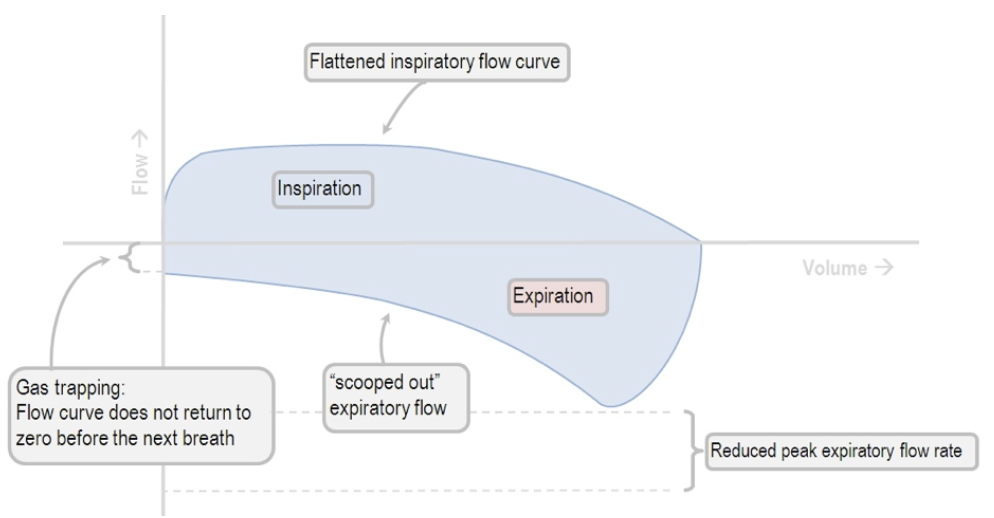
Flow-Volume Loops- yes, the Hamilton can do this. Severe asthma has a very typical Flow-Volume loop and may be useful not only diagnostically but also may identify a failure of the expired volume to return to zero, implying gas trapping, even if the expiratory flow curve is asymptotic
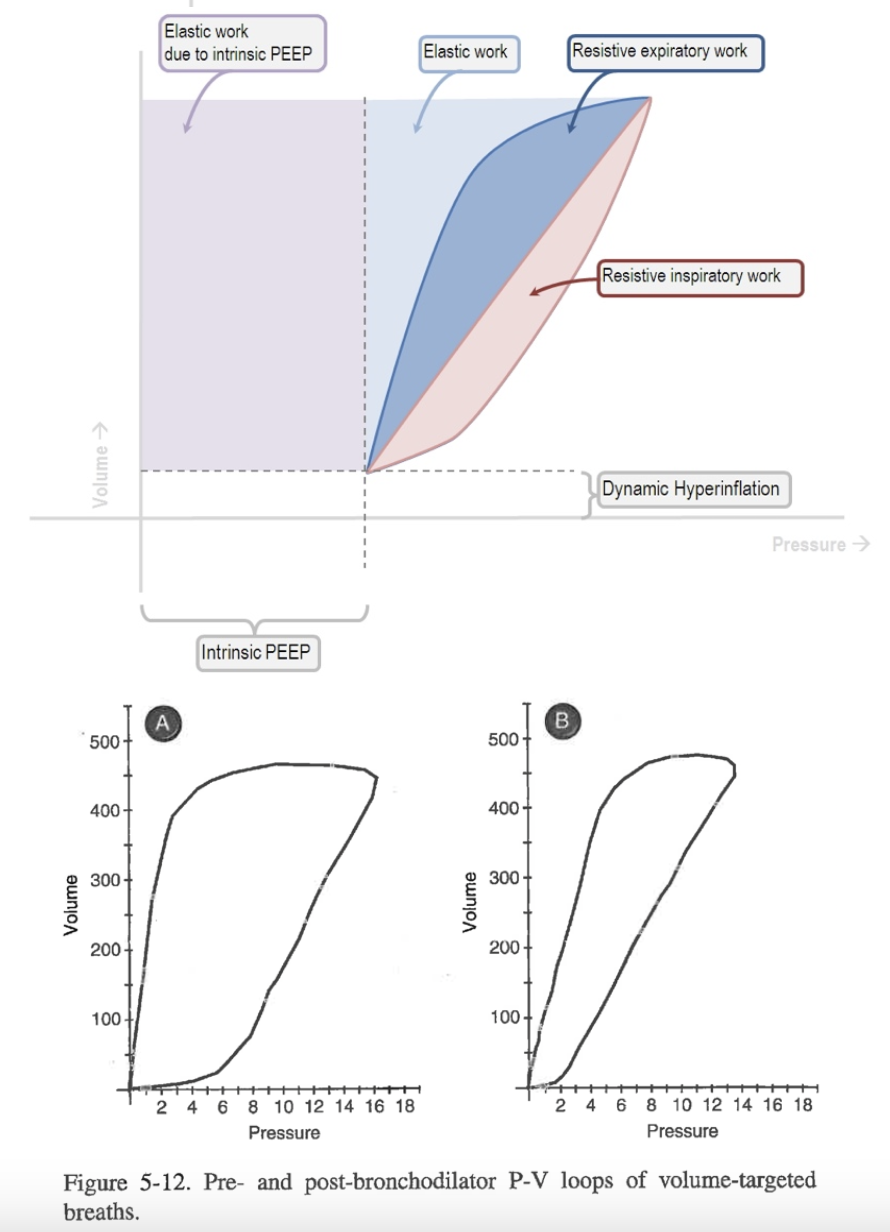
The Pressure-Volume Loop- again, the Hamilton can do this. Expiratory work of breathing is composed of elastic and resistive work of breathing. As bronchospasm worsens, the expiratory resistive work of breathing will increase.
Take Away Messages:
The expiratory flow curve waveform can be valuable for differential diagnoses including large airway obstruction
Use a volume control mode with the Pinsp limit set as high as it can go, provided the plateau pressure is safe
Your ventilatory goals in an asthmatic are: pH >7.2, Plateau pressure <25 and PEEPi <10-12. If the pH is safe, a high CO2 does not matter in stock standard patients.
Low rate, high I:E
Use a multimodal clinical assessment to determine clinical trajectory instead of relying on PaCO2 or just an expiratory flow waveform
If you’re not winning, consider a trip to an operating theatre for volatile anaesthetic or a phone call for ECMO.
Sydney HEMS acknowledges the Australian Aboriginal and Torres Strait Islander peoples as the first inhabitants of the nation and the traditional custodians of the lands where we live, learn and work.







 Consider your options for routes of administration. MDI via T piece is a simple quick way to administer salbutamol, but this job requires someone dedicated to ensuring every dose is received on schedule. Continuous nebulisers are an option, but accidentally tipping the nebuliser is something to be aware of. Even small ICUs frequently stock ultrasonic nebulisers, which theoretically can deliver smaller particles more distally. If you’re not convinced the inhalation route is delivering enough, consider changing to IV. Adrenaline offers a familiar IV alternative and covers you for anaphylaxis you’ve incidentally missed. IV adrenaline boluses are a good.
Consider your options for routes of administration. MDI via T piece is a simple quick way to administer salbutamol, but this job requires someone dedicated to ensuring every dose is received on schedule. Continuous nebulisers are an option, but accidentally tipping the nebuliser is something to be aware of. Even small ICUs frequently stock ultrasonic nebulisers, which theoretically can deliver smaller particles more distally. If you’re not convinced the inhalation route is delivering enough, consider changing to IV. Adrenaline offers a familiar IV alternative and covers you for anaphylaxis you’ve incidentally missed. IV adrenaline boluses are a good. 

 AiR Videos
AiR Videos