
Airway Registry learning points reflect the challenges described and wisdom shared by Sydney HEMS personnel and guests at the Clinical Governance Airway Registry presentations. Cases are discussed non-contemporaneously, anonymised and amalgamated over a time period to draw together unifying take-home messages. Details of specific cases are removed and/or changed, such that any similarity to real-life patients or scenarios is coincidental.
Sydney HEMS is proud of its commitment to excellence in airway management. In 2020, we achieved:
- 400 Intubations
- 377 RSIs
- 1 awake nasal intubation
- 1 primary surgical airway
These learning points form part of our commitments to governance, excellence and education. All CMAC videos are shared under a Creative Commons Licence: Attribution 2.0 Generic. Please familiarise yourself with the terms of the licence before reusing our videos.
To view these videos, you will need this password: AiRblogVideos
The AiR blog posts come from the amazing brain of Dr Clare Hayes-Bradley via the fingertips of Dr Natalie May.
Focus on: Paediatric Intubation
How Deep Is Your Tube?
In this video of a 15kg child we attended following a drowning, there are a couple of really important and useful learning points.
Firstly, the video shows how extensive and troublesome pulmonary oedema can be in these patients. It is certainly something we see commonly; this particular case had involved bystander CPR and even though there was spontaneous respiration by the time our team arrived at the patient – and our pre-oxygenation strategy achieved SpO2 100% – there was copious white frothy fluid in the oropharynx, almost obscuring the cords, and then later seen coming back up the tracheal tube (in the later part of the video). The blade used here with the CMAC is size 4; we have used this blade size successfully in patients as young as 14m of age.

Secondly, the black lines seen just above the cords when the cuff is inflated (image below) might appear to be the lines corresponding to the cuff end of the tube but in fact these are the markings at 10cm of insertion – and in this case, this resulted in a right mainstem intubation.


Arrival CXR from hospital (12:25) is shown with a left sided white-out and clear bronchial tube. This resolves once the tube is pulled back (16:14).
Our Paediatric quick reference cards give an ideal depth of tube insertion by age. This is a handy guide to help avoid this common problem and we recommend confirming tube depth (given as ETT length) at the teeth/lips as soon as practical after intubation.

You can find the Paediatric Emergency Reference cards via the ITIM app.
Video Focus on: Airway Soiling & SALAD
With the case above in mind, it’s helpful to remember that we often deal with significant airway soiling. Our service carries the DuCanto suction catheter and trains for suction assisted laryngoscopy airway decontamination (SALAD).
These two videos show significant soiling.
This video shows significant soiling, presumably from gastric contents, during laryngoscopy.
This video, like the one above, shows significant airway soiling. Suction was used continuously (the SALAD technique) to provide a view in order to secure the airway in difficult circumstances.
Further CMAC Videos:
Very Pale Mucosa in a Hypovolaemic Trauma Patient
This video is notable for the significant pallor in the airway mucosa. This was a trauma patient with considerable hypovolaemia.
Unexpected Difficult View
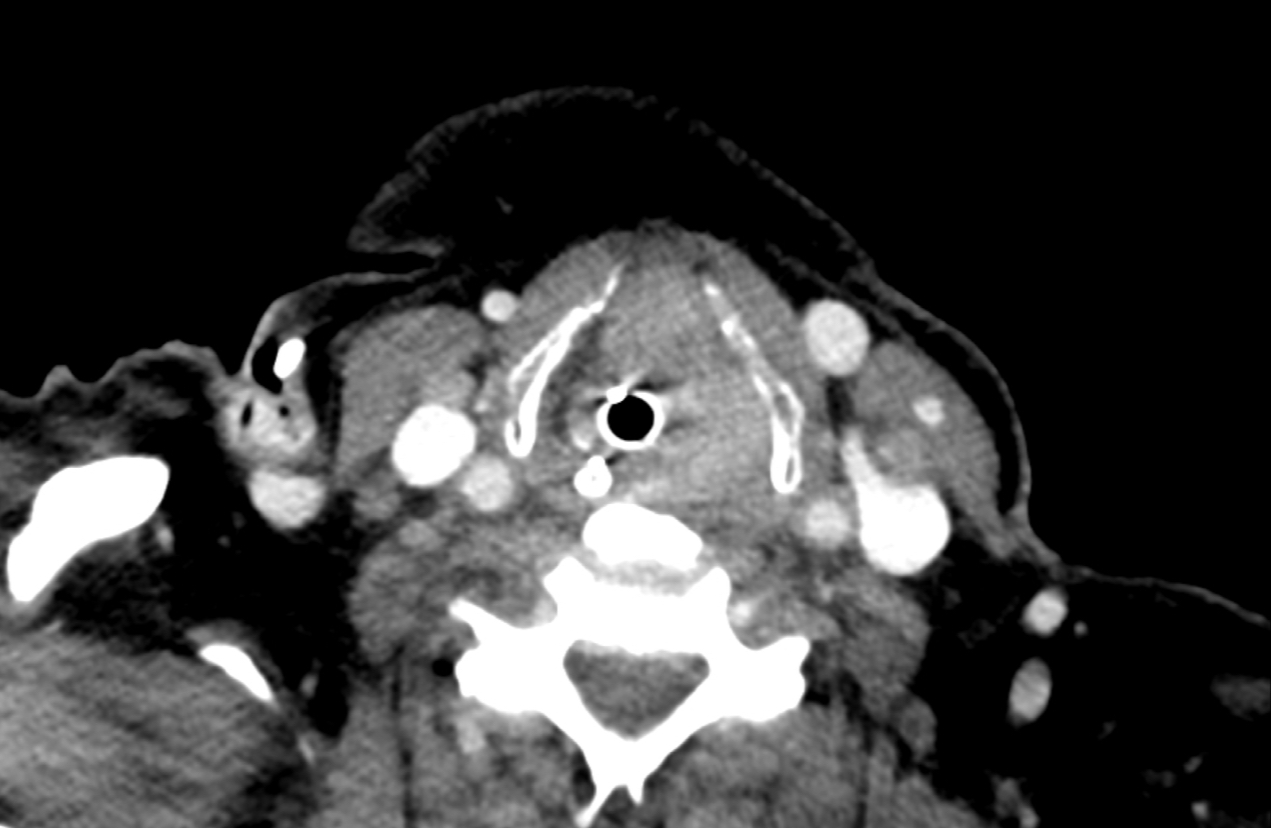
This patient had an unexpected supraglottic mass, making laryngoscopy difficult. The epiglottis is swollen and surrounded by inflamed and friable tissues.
This patient was intubated successfully by the team and the CT scan image is shown below.
CMAC Size 4 Blade in a 2 Year Old
Another example of the successful use of the CMAC size 4 blade in a small child – in this video the patient is 2 years old.
You can see all the AiR videos here on our Vimeo page.


Pingback: AiR – Learning from the Airway Registry (September 2021) – Greater Sydney Area HEMS – Prehospital and Retrieval Medicine – THE PHARM dedicated to the memory of Dr John Hinds