
Intubations this May: 31
Intubations this June: 28
Airway Registry learning points reflect the challenges described and wisdom shared by Sydney HEMS personnel and guests at the Clinical Governance Airway Registry presentations for May & June 2018. Cases are discussed non-contemporaneously, anonymised and amalgamated over a time period to draw together unifying take-home messages. Details of specific cases are removed and/or changed, such that any similarity to real-life patients or scenarios is coincidental.
All CMAC videos are shared under a Creative Commons Licence: Attribution 2.0 Generic. Please familiarise yourself with the terms of the licence before reusing our videos.
To view these videos, you will need this password: AiRblogVideos
Focus on: Getting Stuck
In May we reviewed some videos to talk about how our intubation equipment – bougie or ETT – can get stuck, and what we can do about it.
Stuck bougie
This patient has been exposed to fire/flames with a presumed inhalational injury – note sooty secretions and swollen arytenoids/posterior glottis structures.
We can see the blue (coudé-tip) bougie passes the cords but following that there is resistance to further advancement – seen as the glottis being moved by attempts to advance the bougie. The team remove the blue bougie and use the white bougie which is less curved.
Problem:
The coudé tip is likely impacting on the tracheal cartilages of the anterior tracheal wall.
This is more common with hyperangulated video laryngoscopy but occurs here with a Mac shaped blade.
Solutions:
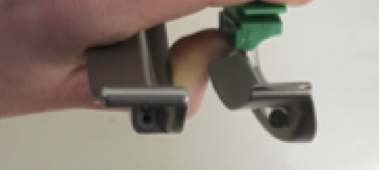
- Rotate the bougie (twist it) to disimpact the coudé tip from the anterior wall
- Reshape the bougie to lessen the tip
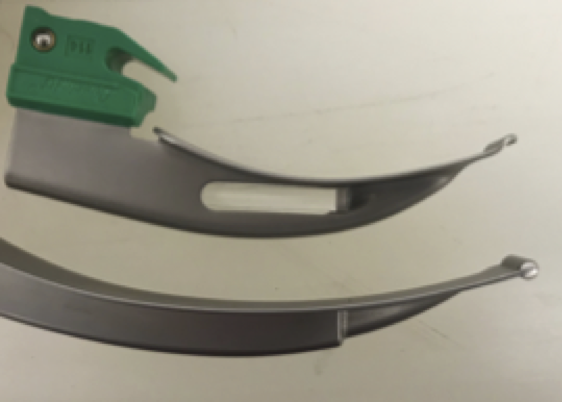
- Exchanged the coudé-tip bougie for a straighter bougie (as was done here – we carry a non-coudé-tip white bougie in addition to the blue bougie).
Stuck tube
We use Parker Flex-TipR ‘GlideRiteTM’ tracheal tubes to reduce the potential for the leading edge of the endotracheal tube to ‘catch’ on glottic structures while railroading over a bougie, as is classically described for the arytenoid cartilages.
This video shows the gap that can exist between bougie and ETT tip that could lead to ‘catch’ (risking failure to advance and laryngeal trauma).
Other discussions
Identifying airway anatomy
This CMAC video is a great example of how the oesophageal inlet can look a lot like a trachea – re-emphasising the need to see arytenoids cartilages in order to positively identify the trachea prior to passing a bougie or ETT.
Soiled airway in cardiac arrest
A medical cardiac arrest can present healthcare workers with an airway flooded with gastric contents. Such soiling can be particulate and thick which can block common Yankauer suckers.
A work-around can be to remove the blocked Yankauer sucker and simply use the end of the suction hosing itself. The hosing is a much larger diameter and is often very successful at clearing the pharynx when used directly.
Be aware that small portable units may have a volume capacity that can be easily exceeded by large volumes of soiling; vehicle-based suction units have a larger capacity.
At Sydney HEMS we carry a longer suction tubing set so we can connect to the in-ambulance vehicle suction while intubating at the back of the ambulance.
Video Focus on: two learning points from one video
This CMAC video from June has two separate learning points! The learning points below both refer to this CMAC video:
1. Dry mouth
Patients who have spent some time prior to intubation breathing non-humidified wall O2 (for example, via a non-rebreathe mask) can have very dry mucosa in their oral cavity on airway assessment. An assessment of the dryness of oral mucosa is not classically part of a pre-intubation airway assessment but it can cause issues, so it is important to notice. Pre-lubricating the blade can make the laryngoscopy much easier; lubricating gel can be Lseen on the blade in this video.
You might remember similar “dry mouth” issues from this earlier CMAC video:
2. DL to VL
Initial attempts to intubate this patient were made using a direct laryngoscopy technique. During DL, the operator struggled to identify the inter-arytenoid notch landmark. The intubator proceeded to use the video screen (VL technique) which gave them a clearer view of the glottis and allowed placement of the bougie.
It became evident that a sputum plug was obscuring the inter-arytenoid notch landmark that the operator had been trying to visualise. Having the back-up of video laryngoscopy on this Mac 4 blade intubation was very useful.
You can see all the AiR videos here on our Vimeo page or here on the blog.







 AiR Videos
AiR Videos