
Another excellent clinical governance day for the Sydney HEMS team where we got down and dirty with trauma-induced coagulopathy, how to deal with maxillofacial haemorrhage, tools used to plug the gaps, a recollection of epic winching, and a Sim that got us all bloody!
Winch Audit – Cameron Edgar
Cameron went through the logistics of a particularly complex winch mission that involved a 70 meter abseil down to a cliff-edge followed by a 130 meter patient-accompanied abseil to ground! With most pre-hospital cases, the team has to plan for the following:
- Access
- Triaging
- Treating
- Evacuation
Flexibility in our clinical practice means that logistics can sometimes affect the priority of patient management.
Check out this video (courtesy of Timothy Sharman) of a previous winch job to give an idea of the limited access and difficulties in treating and evacuating patients on a complex mission.
TIC Tactics – Phil
Trauma-induced Coagulopathy (TIC)
Phil went through the latest thinking on what trauma-induced coagulopathy (TIC) is, why it matters and what we can do about it!
- TIC is much more complex than just a loss or dilution of clotting factors
- TIC occurs because of a combination of acute-traumatic coagulopathy (ATC) and what we do…

There is a collective imbalance, a dynamic equilibrium that gets broken rather than just a loss of clotting factors – and this can happen rapidly
ATC
This is a series of physiological changes affecting the clotting cascade that requires both tissue trauma and hypoperfusion to exist. Patients presenting with ATC on admission seem to have worse outcomes. It occurs because of the following:
- Low fibrinogen with increased fibrinogenolysis
- Factor V deficiency causing procoagulant impairment.
- Occurs within 25 minutes of a traumatic injury in 56% of patients.
- Strong activation of Protein C
- Platelet count reduction and functional disturbance
- Vascular endothelium changes – protein C activation, t-PA inhibitor consumption (self-thrombolysis) and auto-heparinisation
What we do!
Our management may support development of TIC:
- High volumes of crystalloids (>3 litres)
- Hypothermia (<33ºC)
- Acidosis (pH 7.2)
What should we do?
- Damage control resuscitation!
- Early tranexamic acid (avoid 3 hours post-trauma due to a paradoxical increased mortality)
- Keep them warm
- Avoid acidosis
- Blood and clotting product replacement
Remember the following doses:
- FFP – 15ml/kg
- Cryoprecipitate 3-4g
- Platelets 1 adult therapeutic dose
Check out the following reference for more information:
Frith D, Brohi K. The pathophysiology of trauma-induced coagulopathy. Curr Opin Crit Care. 2012 Dec;18(6):631-6. doi: 10.1097/MCC.0b013e3283599ab9. Review. PubMed PMID: 23010636
Blood from the Floor – Sameer
Pre-hospital management of maxillofacial haemorrhage
Sameer discussed an interesting case he managed where a patient sustaining significant traumatic maxillofacial injuries. In this situation, he had 2 management priorities:
- Avoid asphyxia – secure the airway
- Avoid exsanguination – stop the bleeding
We talked about intubating airway and maxillofacial bleeds last week, but how do you achieve haemorrhage control? Our kit for maxillofacial trauma includes the following:
1. McKesson dental props – To be placed between top & bottom teeth, thereby pushes the midface up towards base of skull, thus reducing the fracture and assisting in haemorrhage control. Note that this is not useful when used with mandibular injury unless C-collar on first to support the mandible.

2. Nasal epistat catheters – Insert parallel to the floor of the mouth as with a nasopharyngeal airway. Comprised of two balloons:

Inflated with 10ml to the posterior balloon and 30ml to the anterior balloon
- A posterior balloon (10ml volume) to be inflated first
- An anterior balloon (30ml volume) to be inflated second
These are extremely useful devices as they allow patients to breath through the central lumen. There is obviously a rare risk of inappropriate placement with head and maxillofacial injuries, thus care in their insertion must be used and a suggestion of aiming towards the centre of the occiput (regardless of the facial displacement) with the catheters might reduce any unwanted complications.
So what are the steps of managing a patient with a maxillofacial trauma?
1. Intubate, confirm ETT placement – wait to tie the tube! Tube tie may impair McKesson dental prop placement…
2. Apply cervical collar
3. Attempt manual reduction of the midface
4. Insert nasal epistats – don’t inflate yet
5. Insert McKesson dental props
6. Inflate the nasal epistats – slowly with a few mls in each epistat, posterior balloons first!
7. Tie the ETT
8. Get to hospital
Plugging the Gaps – Carla
Foley catheters, Sengstaken-Blakemore tubes and REBOA
Carla gave us an excellent rundown of the tools we can use to plug the gaps in those bleeding tubes!
Foley balloon catheter
On of the most useful devices in modern medicine, Carla talked about the situations we might use them in the pre-hospital trauma environment:
- Penetrating cardiac wounds – can insert a Foley catheter directly in to cardiac wound and inflate with 5ml normal saline. Pitfalls – bleeding can continue around margin, traction can extend the wound, reduce cardiac output by occupying intramural space!
- Penetrating neck trauma – successfully used in South Africa extensively
Sengstaken-Blakemore tubes/Minnesota tubes
These devices also use a balloon tamponade technique for short term haemostasis. Have a look at Scott Weingarts How-To of SB Tubes:
GI BLEEDING TIP 1
In the transit (helicopter or ambulance), the best method to provide stable traction where the tension on the SB/Minnesota tube not affected by bumps, acceleration and deceleration is:
 Image from Eur J Emerg Med. 2013 Apr;20(2):144-5
Image from Eur J Emerg Med. 2013 Apr;20(2):144-5

Apply a cervical spine collar to the patient, then tie the SB/Minnesota tube to the collar using ETT tying tape to provide traction
GI BLEEDING TIP 2
If you are trying to intubate a patient with active upper GI bleeding, then you can place an ETT into the oesophagus, clamp it and inflate the balloon. This will prevent further bleeding from getting in your line of sight, so you can then suction the airway and intubate. The alternative is a digital intubation (feel the epiglottis with your fingers and blind bougie).
REBOA
Resuscitative endovascular balloon occlusion of the aorta (REBOA) is a resuscitative adjunct allowing you to occlude either thoracic aorta or infra-renal aorta with an aortic balloon device. This is surprisingly old technique is making a resurgence. The descending aorta comprises three zones in which the balloon can sit:
1. Thoracic aorta – Zone occluded for non-compressible torso haemorrhage control
2. Aortic Branches – NON-OCCLUSION ZONE
3. From lowest renal artery to aortic bifurcation – Zone occluded for pelvic haemorrhage that is uncontrollable
Image from J Trauma. 2011 Dec;71(6):1869-72
It is still early days in the pre-hospital use of this technique, but have a look at the Shock Trauma Center (STC) protocol on REBOA and the fantastic post and podcast by Scott Weingart:
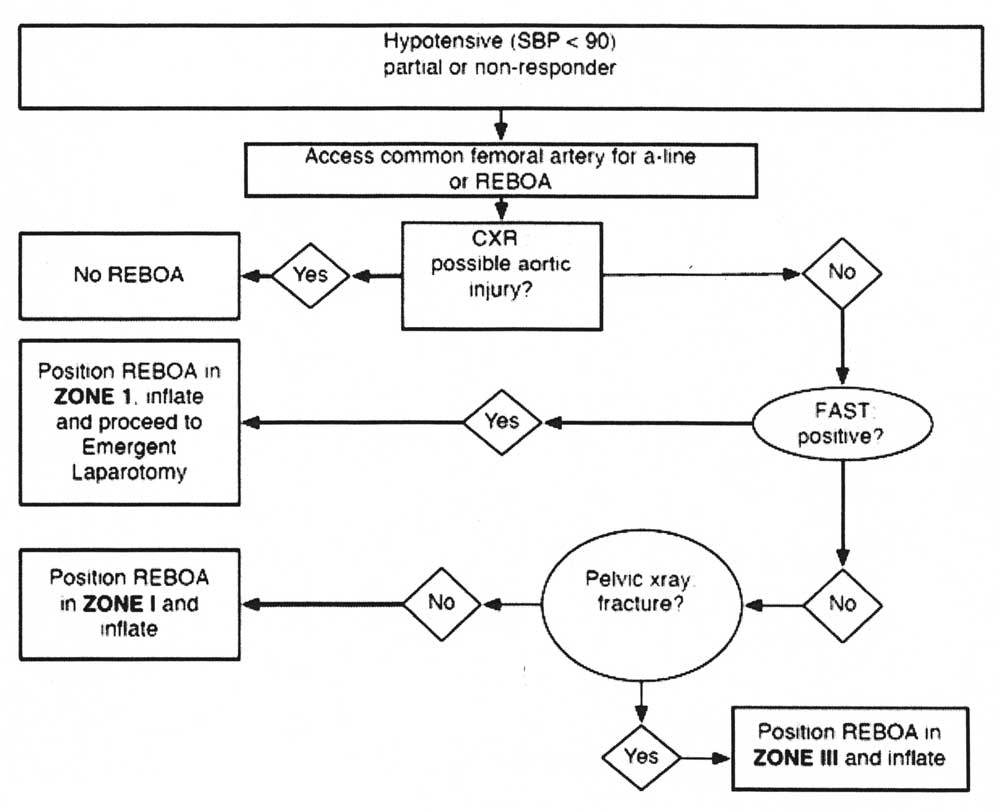
Image from the STC REBOA Protocol
SIMS!
One of the new Sydney HEMS Registrars was given a welcome of fire to manage a patient with a traumatic limb amputation and maxillofacial bleeding. He applied the teaching points we learned on the day so far, but other key messages to take away include:
- In major haemorrhagic trauma, use the approach of ‘CABC’ for obvious bleeding points
- Aim for early extrication in order to fully assess and achieve 360 degree access
- Beware of lying patient on their back with maxillofacial injuries as this may lead to airway obstruction
- Suxamethonium dosing: 2mg/kg in shock is what you should be aiming for
- Always expose and assess for further bleeding points other than the obvious ones – being systematic is the best way to avoid this pitfall
- Maximal simultaneous activity and graded assertiveness are skills that we should all be developing for difficult and complex scenarios we are likely to face



Pingback: The LITFL Review 136 - LITFL