
A high fidelity simulation in the AW 139 aircraft.
The lead -in
15-year-old male with a stab wound
Scene
The initial assessment was performed at a scene outside pub.
The patient
A – Patent
B – RR 32, sats 96% on high-flow O2, bilateral equal airway entry
Chest USS revealed a haemo-pneumothorax on the left side. There was evidence of a 2cm stab wound with a small amount of ooze
C – HR 120bpm sinus tachycardia, BP 112/56. IV access present with a palpabable radial pulse and no other stab wounds noted
D – E4 M6 V4, pupils equal and reactive, smells of alcohol. There were no external signs of head injury and the patient was co-operative
E – No extremity injuries noted
Initial plan: package the patient for a 30-minute air transfer to the children’s hospital (a major trauma centre).
In flight the patient develops PEA cardiac arrest 15 minutes from hospital…
Questions to ask yourself at this point:
Do you land or continue to destination? What guides this decision?
How can space/access to the patient be improved in the AW 139?
Traumatic cardiac arrest and clamshell thoracotomy in flight: really?!
There are crucial CRM points to consider between the doctor/crewman/pilot/paramedic; how would you manage these?
Scenario Progress
Decision was made to land.
Traumatic cardiac arrest protocol was followed in-flight and on ground.
Cold intubation of the patient was difficult due to limited access. The patient was positioned north-south in the helicopter.
3 units of blood given, bilateral thoracostomies performed but patient remained in cardiac arrest.
Cardiac ultrasound revealed cardiac standstill and evidence of cardiac tamponade with clots.
Clamshell thoracotomy performed in the back of helicopter with relief of cardiac tamponade and ROSC.
Post-procedure sedation, paralysis and TXA was given.
Learning points
- Always strive to improve access around your patient. In the AW 139, you can achieve this by:
- Move paramedic’s and doctor’s seats as far back in the cabin as possible facing forward and fold rear seats up (see representation below).
- Move patient stretcher a further 6cm south, moving secured equipment if required.
- Come off seatbelt and on to wander lead early
- Anticipate clinical demise of patients! Get the surgical bag (red loaf) out of the primary pack (blue) and keep nearby
- If you want to free up your hands for clinical activity ‘hot mic’ between doctor and paramaedic
- CRM can help you make decisions. Discuss difficult problems with all your crew.
- Don’t forget eye protection for all surgical procedures
- To land or not to land: This is multifactorial depending on expected arrival to destination and aviation factors (weather, availability of landing sites).
- PRO – Frees up crewman and pilot to aid with fast/efficient treatment of the patient.
- CON – Time critical lesion requiring definitive surgery
Again: ANTICIPATE THE CLINICAL DEMISE OF YOUR PATIENTS!
Management of traumatic cardiac arrest can be found on the HOPs here, with an excellent review of management found here.
Thanks to Matt (Doctor), Phil (ICP), Pat (Crewman), Carla (STAR, Sim controller), Alex (Scenario orchestrator) Cliff (debriefer) and Bubba & Lucas (Experiential insight-providers).
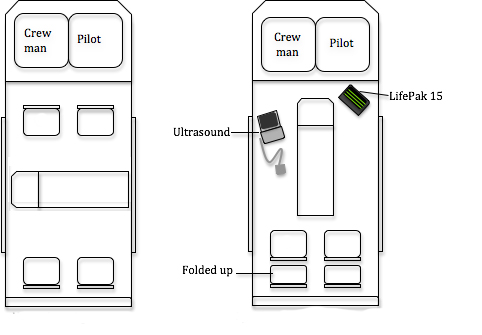
Standard configuration (left) vs space-optimised configuration (right)

AW 139 space difficulties

