
Chris “Willko” Wilkinson (SCAT paramedic) shared this handy trick of the trade during a recent simulation session.
Scenario
Road primary job to a school where a 6 year old girl is in severe respiratory distress with known asthma. On arrival sats are 85% on a non rebreather, RR40, poor air entry bilaterally and responding only to pain. Minimal response to IM adrenaline (Review of adrenaline in asthma)
Airway secured by rapid sequence intubation. We see a good CO2 trace but she is very hard to bag.
Question
How can we deliver salbutamol to the bronchioles of this patient in the prehospital setting?
Options in our kit:
- Salbutamol metered dose inhaler but patient is intubated
- 5mg IV salbutamol but no infusion pump.
- 5 x 5mg salbutamol nebules but no T-piece in our interhospital pack.
Materials

- Sabutamol Metered Dose Inhaler
- 30ml Syringe
- Patient connector with suction port from an Adult Oxylog 3000 disposable circuit
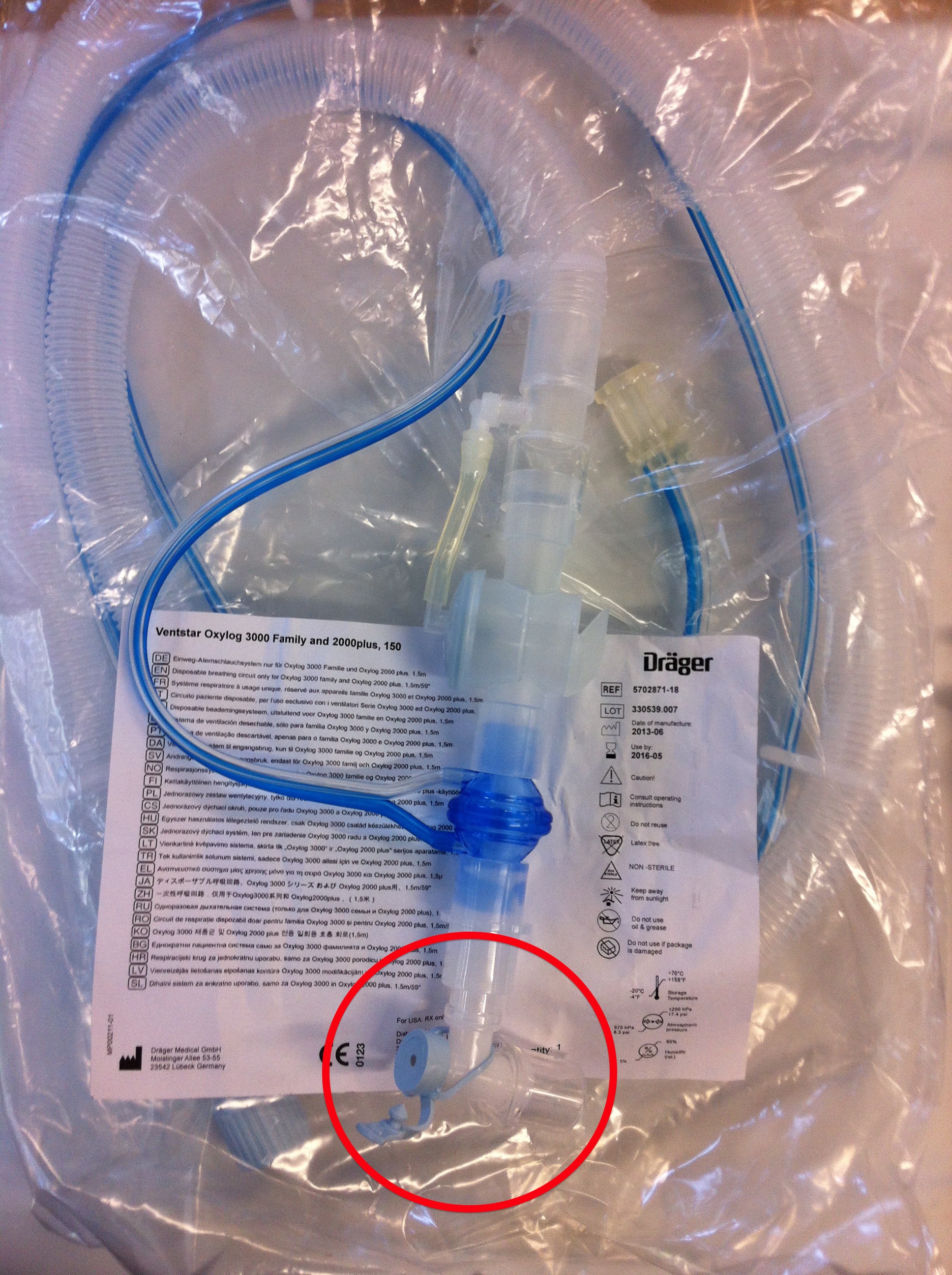
The patient connector is the most distal piece from an adult Oxylog 3000 disposable circuit.
Putting it together

- Attach the Oxylog patient connector to the ETT and continue bagging the patient SLOWLY (to prevent hyperinflation)
- Pull the plunger out of the syringe
- Put the Salbutamol cartridge in the syringe barrel and replace the plunger
- Spray salbutamol through the suction port of the oxylog patient connector in synchrony with bagging
Here’s a 2 minute video showing how to do it in real time
IV Salbutamol
A bolus dose is 10mcg/kg every 15min (critical care drugs)
That’s 250mcg in this 25kg 6 year old. So we could dilute 5mg in 50ml giving us 5omcg/ml and bolus 5ml every 15min.
The infusion dose is 5-10 mcg/kg/min (RCH drug doses online).
So if we put 5mg in 250ml of saline and run it in over 20 minutes we will be getting about 250mcg/min but our transport time may be longer than this and we run a greater risk of causing hypokalaemia.
However the evidence for IV salbutamol is not great and some question whether we should be using it at all. Nonetheless I would probably use it for this child IF I could find the dose, figure out an appropriate dilution and run it at a safe rate without the aid of an infusion pump. A review of the management of life threatening asthma was recently published in the British Journal of Anaesthesia


Great to know how to “McGiver” something out on the road for the MDI. Also it shows how difficult paediatric calculations can be – 5mg in 50ml would equal 100mcg/ml?
Please keep the tips and tricks coming.
The difficulty of paediatric drug dosing in the heat of the moment is well recognized. I guess thats why we carry a pediatric dosing chart printed in big font. Unfortunately, IV salbutamol isn’t on it because it is so rarely required. There are a few phone apps like Frank Shanns Drug Doses that can help.
Nice idea – he come up with thus at spur of the moment? We carry a tpiece and 5x5mg salbutamol nebs but no iv salbutamol… Can only remember ever using it one in hospital practice – have I just been lucky?
Reading the review with interest.
No it wasn’t spur of the moment Wilko says he has used it more than once in the field.
As for IV salbutamol I’ve used it quite frequently in ICU with refractory asthma. That said I think there has been a decreased incidence of life threatening asthma presentations in Sydney. Perhaps due to better prevention?
How much of the dose is actually delivered rather than adheres to the insides of the tube? Probably more than is inhaled without a spacer I guess…
Could it be delivered into the bag of bvm?
It needs to be synchronized with ventilation in order to get decent delivery to the airways. If you synch well the delivery is probably as good as a spacer. Many ICU ventilator circuits have dedicated ports for MDI’s and giving drug through these seems to work in my experience.
We carry something like this. While I’m sure that would work, having the correct kit in the first place is much simpler.
http://extww02a.cardinal.com/us/en/distributedproducts/ASP/HS762.asp?cat=med_surg
I agree, having the right kit is always the best option where possible. However, the scenario of a crashing asthmatic who requires intubation and ventilation prehospital is so rare that it would be hard to justify having a dedicated piece of kit
excellent idea