
Airway Registry learning points reflect the challenges described and wisdom shared by Sydney HEMS personnel and guests at the Clinical Governance Airway Registry presentations. Cases are discussed non-contemporaneously, anonymised and amalgamated over a time period to draw together unifying take-home messages. Details of specific cases are removed and/or changed, such that any similarity to real-life patients or scenarios is coincidental.
Sydney HEMS is proud of its commitment to excellence in airway management. In 2018, we achieved:
387 Intubations
352 RSIs
96.5% First look laryngoscopy success at RSI.
These learning points form part of our commitments to governance, excellence and education. All CMAC videos are shared under a Creative Commons Licence: Attribution 2.0 Generic. Please familiarise yourself with the terms of the licence before reusing our videos.
To view these videos, you will need this password: AiRblogVideos
Focus on: CMAC Screen Issues
Fogging of the CMAC Screen
Fogging of the CMAC pocket monitor screen at laryngoscopy is commonly seen and can last 20-25 secs before it clears. One video which runs for 2m30s before laryngoscopy shows that turning the screen on during the checklist phase of preparation for intubation does not always prevent the fogging from occurring. It doesn’t always completely obscure the view but can make it tricky, so it’s something to be aware of.
Why is it so Dark?!
Observation from one team member:
“My view of the CMAC screen was very dark when undertaking intubation (it had been fine when it was checked during the checklist phase). Only after intubation did I realise this was due to my polarised sunglasses!”
Other Topics of Discussion
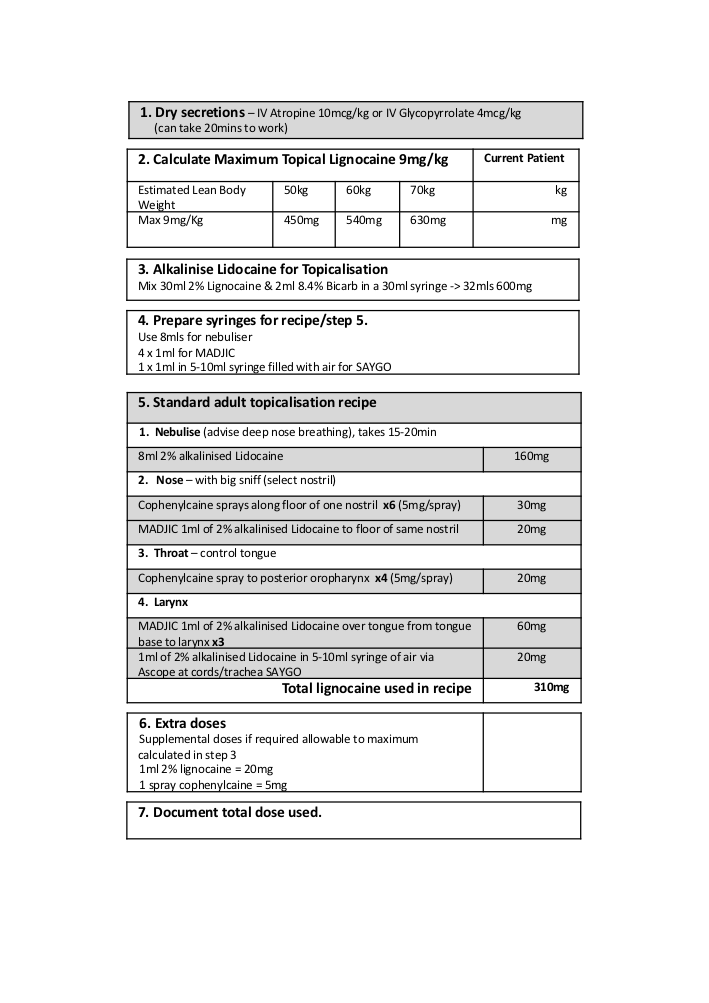
A few months back we had our first awake fiberoptic nasal intubation of 2019 – and received helpful feedback that the new look topicalisation recipe was successful (see below).
Video Focus on: Contaminated Airways
We see many examples of airway contaminants, particularly during our prehospital missions but also during interhospital transfers. Some examples are shared below.
Dry Mucosa and Sputum
Dry mucosa and sputum are evident in this video from a patient with community acquired pneumonia and dehydration.
Burned Airway
This patient was trapped in a burning vehicle for some time.
Immersion – Frothy Airway
Any patient who is retrieved from water should be thought of as being at risk of immersion and near drowning pulmonary oedema.
Thick Secretions
This video from a patient with sepsis shows thickened oropharyngeal secretions.
Brown Goo – A Diagnostic Laryngoscopy?
This video shows intubation in a very sick patient with pneumomediastinum of unknown cause – at intubation oropharyngeal infection and abscess were apparent with fluid oozing from the epiglottis at laryngoscopy.
Further CMAC Videos:
Release the ELM!
In both of these cases, external laryngeal manipulation (ELM) was initially used to ‘improve’ the view at laryngoscopy. The video of ELM being released shows how ELM can actually make the view worse.
When performing ELM in the role of airway assistant, always get feedback from the laryngoscopist as to whether the ELM is helping – and when available the video screen may help aid ELM placement by the assistant. Both of the efforts seen on video here may be too high in the neck, resulting in pressure above the glottis.
Tracheomalacia – Seen Using Ambu A Scope via Tracheostomy
This video is from the A View monitor of the Ambu A Scope and shows the regular 5.0mm diameter scope placed into 7.0mm tracheostomy, demonstrating tracheomalacia – the floppy trachea collapses down on expiration and opens on inspiration. This was a great use of a bedside tool to demonstrate pathology and contributed to patient care.
You can see all the AiR videos here on our Vimeo page or here on the blog.


Hello, great resources!
I would be interested in how you record with your videolaryngoscope
Regards
Claudio
Hi Claudio,
We use the CMAC (R) pocket monitor, produced by Karl Storz. It has inbuilt recording capability – you can find out more here: https://www.karlstorz.com/cps/rde/xbcr/karlstorz_assets/ASSETS/3327720.pdf
I would suggest contacting Karl Storz with further enquiries. Thanks!
Natalie