
Airway Registry learning points reflect the challenges described and wisdom shared by Sydney HEMS personnel and guests at the Clinical Governance Airway Registry presentations. Cases are discussed non-contemporaneously, anonymised and amalgamated over a time period to draw together unifying take-home messages. Details of specific cases are removed and/or changed, such that any similarity to real-life patients or scenarios is coincidental.
Sydney HEMS is proud of its commitment to excellence in airway management. In 2018, we achieved:
387 Intubations
352 RSIs
96.5% First look laryngoscopy success at RSI.
These learning points form part of our commitments to governance, excellence and education. All CMAC videos are shared under a Creative Commons Licence: Attribution 2.0 Generic. Please familiarise yourself with the terms of the licence before reusing our videos.
To view these videos, you will need this password: AiRblogVideos
Focus on: Cold Intubation
For patients in cardiac arrest, we generally omit our longer pre-intubation checklist as well as RSI drugs – but we do not intubate without anychecklist. Instead, we use a “cold intubation” checklist – a shorter version, printed on the reverse of our standard RSI checklist card and designed to help remind teams of the common mishaps encountered in cold intubation attempts. Ideally, attempts to oxygenate an arrested patient should continue whilst position is optimised and equipment e.g. EtCO2 are sought.

Other Discussions
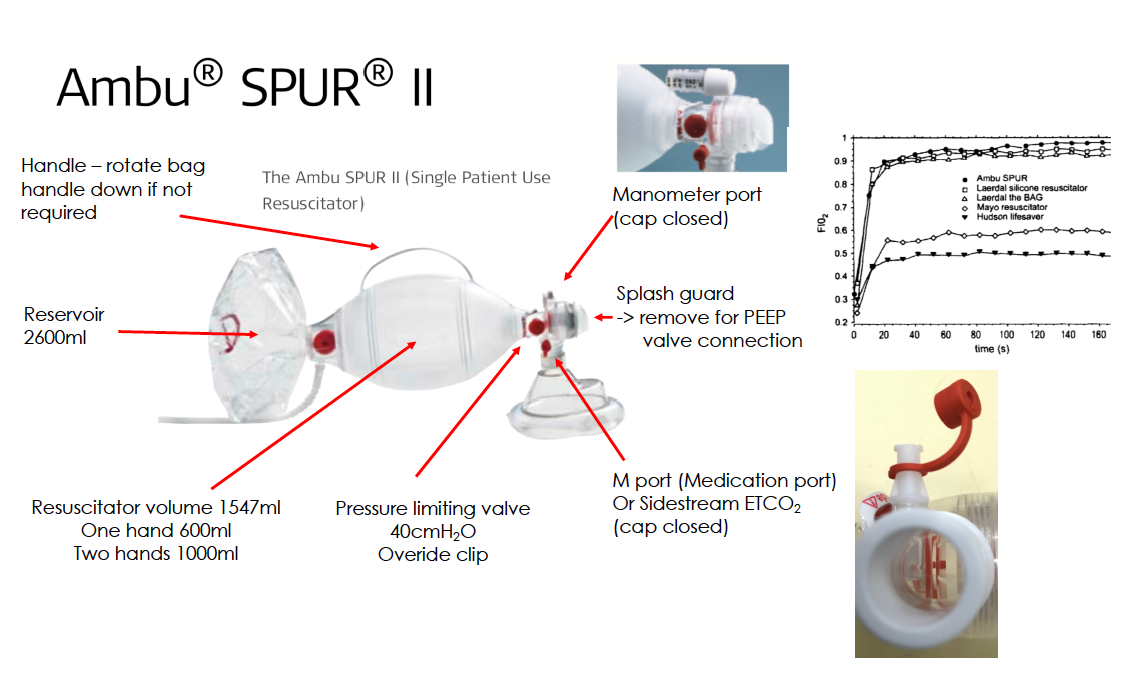
New AMBU SPUR II – “single patient use resuscitator”
These resuscitation bags are now carried by NSWAmbulance – the following PDF is a summary of the company literature. Of note, with spontaneous ventilation, there is no air entrainment via the exhalation valve giving a high FiO2. There are two ports that could be a source of leaks and need their caps in place (M port & Medication port). The PEEP valve fits on the exhalation valve as previously.
Cuff leak & ETCO2
After intubation the presence of EtCO2 waveform may depend on the inflation of the cuff. If EtCO2 does not appear, it is worth having a quick check of the cuff pilot balloon before concluding that the ETT is misplaced. Cuff deflation, obstructed ETT/trachea and extreme bronchospasm have all been seen by our team as causes of an absent ETCO2 waveform.
Video Focus on: Bougie Benefits – and Bothers
In our service, we routinely carry a white (straight-tipped) and a blue bougie. We allow our teams to decide which of the two is used (although our standard practice is to use a bougie for every intubation) and both have benefits and downfalls, as explained below.
Ambient Temperature: Bendy or Brittle?
The Sydney sunshine can make our blue bougies become warm and floppy this time of year. Conversely, we regularly hear from the Orange base, that winter make the white bougies unbendable. This may influence choice of bougie during RSI setup.
Bougie Tips
In this laryngoscopy video, the cords appear in the upper portion of the video screen (and the epiglottis is lifted directly). Our straight tipped white bougie cannot be redirected to the upper screen. Our blue bougie with the Coude tip is more suited to this view.
Right for Rings
Above is some good footage of a bougie catching on anterior tracheal rings along with successful rightward rotation to disconnect from rings. “Right for Rings”, as people say.
Twenty Seconds to Pass the ETT
And finally, one for the bougie-sceptics: in this CMAC video, one of our paramedics shows that even using our standard ETT-over-bougie technique, the ETT cuff can be past the cords within 20 seconds of starting laryngoscopy.
Further CMAC Videos:
ETT Catching the Cords & ETT Catching the Epiglottis
Another two examples of how any tube can potentially catch when railroading over a bougie and the need to ‘detect catch and stop, withdraw slightly and turn 90 degrees anticlockwise’ still exists. Some practitioners will automatically turn 90 anticlockwise when feeding an ETT over a bougie to avoid this catch (as it closes the gap between ETT & bougie).
ELM Closing the Cords
External laryngeal manipulation (ELM) can act to ‘pinch cords together’ and make passing the bougie harder – we would advise an assistant to both look at the video screen and asking the laryngoscopist for feedback while applying ELM.
Really Long Epiglottic Tunnel
This normal variation of epiglottis can be challenging. The long ‘tunnel’ created may appear darkened in a lit room.
You can see all the AiR videos here on our Vimeo page or here on the blog.

