
Intubations this month: 22
Airway Registry learning points reflect the challenges described and wisdom shared by Sydney HEMS personnel and guests at the Clinical Governance Airway Registry presentation for January 2018. Cases are discussed non-contemporaneously, anonymised and amalgamated over a time period to draw together unifying take-home messages. Details of specific cases are removed and/or changed, such that any similarity to real-life patients or scenarios is coincidental.
Focus on: Soiled Airway
The threat of massive airway soiling at laryngoscopy and intubation has troubled airway practitioners for decades; and yet, in 2018 we still don’t have a great evidence based plan of how to approach such threats.
To view this video you will need this password: AiRblogVideos
Discussion points around this challenge include:
- Predictability – in addition to history & examination – could bedside gastric ultrasound assist us with risk assessments when feasible?
- Preparation – practising a ‘SALAD’ sim at the base, and talking through your actions in your airway plan with your team before starting
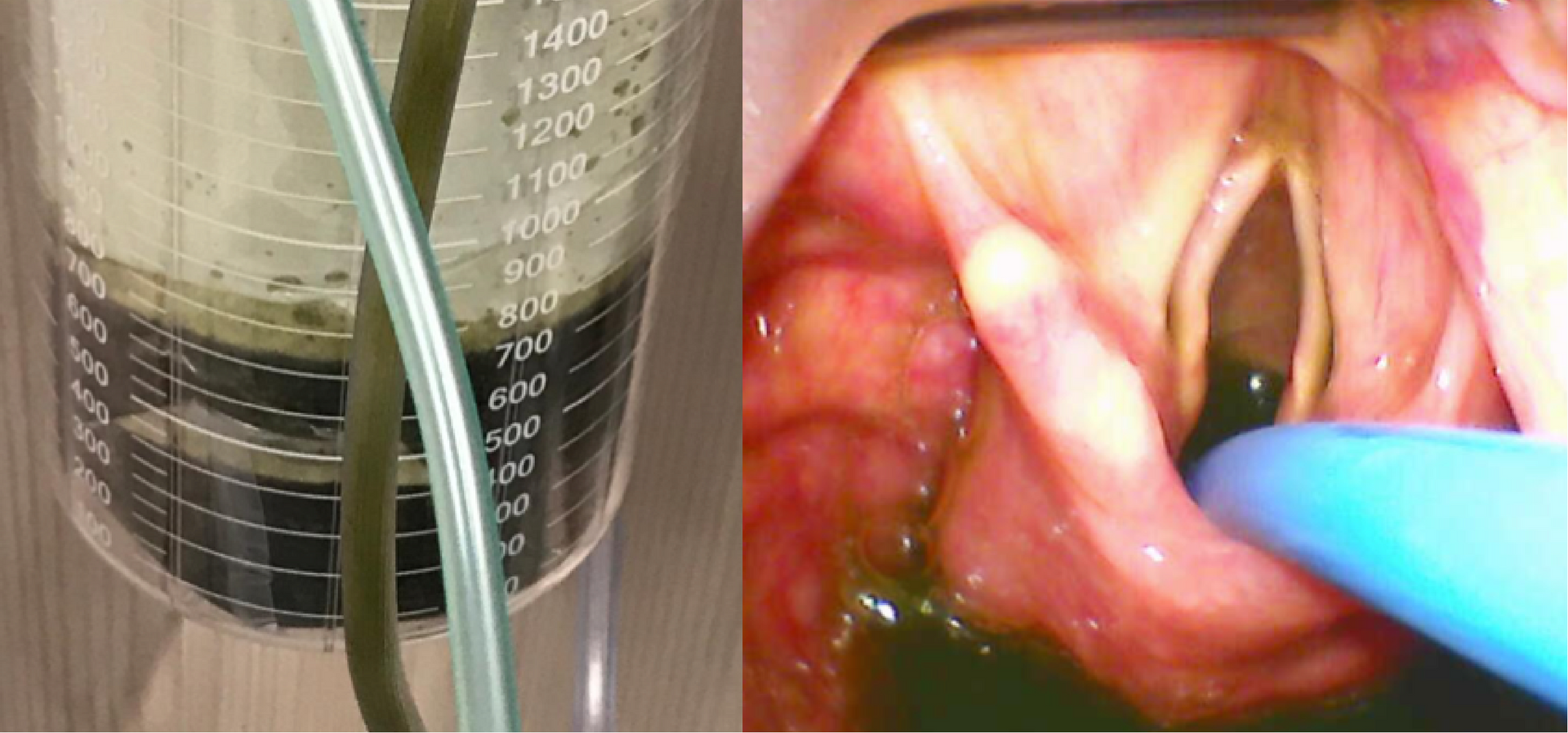
- Drainage – does a gastric tube, when feasible, drain sufficient volume to reduce risk?
- Positioning – but some patients aspirate when fully awake and sitting up
- Awake intubations – very difficult/nigh impossible in the hypoxic and critically ill
- Cricoid pressure – recommended in the ‘Guidelines for the management of tracheal intubation in the critically ill adults’ found here http://bjanaesthesia.org/article/S0007-0912(17)54060-X/fulltext, which states ‘cricoid force advocated, with prompt removal if necessary’.
Other Airway soundbites this month
Laryngospasm after Ketamine
Laryngospasm or apnoea occurring after ketamine sedation can be frightening for the practitioner and is one of the reasons why other prehospital services have ketamine sedation ‘protocols’. Symptoms and signs of laryngospasm witnessed by our service following a small sub-dissociative (<0.5mg/kg) dose for agitation were:
-
- Continuing respiratory effort with see-saw respiratory movements
- Absolute airway obstruction (complete loss of ETCO2 trace from Bag Mask device, loss of fogging and subsequent desaturation).
Actions of 2 person Bag valve mask, Larson’s manoeuvre and increasing sedation resulted in successful ventilation. The subject is further discussed here: http://resus.me/laryngospasm-after-ketamine/
Reoxygenating
Reoxygenating between laryngoscopy attempts can be difficult – OPAs, NPAs and two-person-technique for bag mask ventilation is generally recommended but is challenging for those patients sporting a beard. Solutions suggested have included “plasticising” the beard with tegaderm, but this is rarely practical in the Retrieval setting where airway management is rarely elective.
One alternative to reoxygenate between laryngoscopy attempts is to use our iGel SGA which is not affected by the presence (or absence) of facial hair.
CMAC Caution
Our CMAC pocket monitor laryngoscopes have a built-in ability to turn themselves off (blade light and screen). Manufacturer advice is that this will happen after 10 minutes of no use detected by no change in light intensity at the camera. The device turns on again very quickly by closing and opening the screen. Should this occur during a laryngoscopy, it may be prudent to open and close the screen in situ.
Blade Tip Positioning
Laryngoscope blade tip position is critical to successful laryngoscopy. The following still shots from CMAC Pocket Mac 4 blade videolaryngoscopy show this in action.
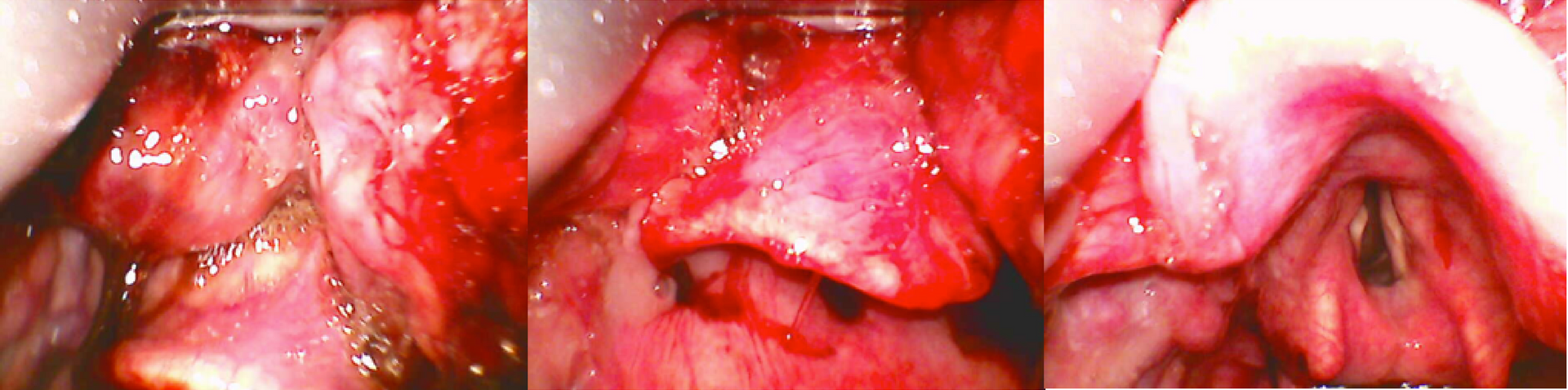
The first image shows the tip sitting high of the vallecula (where the smooth shiny epiglottis mucosa meets the lumpy bumpy tongue). Efforts to lift the epiglottis by lifting the laryngoscope here are unsuccessful resulting in no view of the larynx (Grade 3 view as epiglottis only seen). The middle image shows the tip sitting in the vallecula where indirect epiglottic lift with the laryngoscope is successful revealing the laryngeal inlet (Grade 1 view = POGO 100%).

