
This blog post is an accompaniment to a presentation at the August ’23 Clinical Governance Day. The purpose of the talk was to update the service on the Quality Improvement Project I have been leading on.
Why is C+C important?
– There is something to learn from every case – especially when your caseload is predominantly high acuity – such as in a HEMS service.
– In contrast to hospital life, we work in relative isolation in HEMS. Of course, we are always part of a two-person team, but opportunities for doctors and CCPs to receive direct observational feedback from colleagues from the same discipline are perishingly rare. Regular case-based discussion is the next best thing.
– It is an education platform alongside a safe space for debrief, camaraderie and pastoral care.
– It dovetails beautifully with our governance process. Cases warranting further exploration can be flagged to the right governance team (e.g. M+M, airway audit etc) to ensure they haven’t been missed.
Why does it work so well?
– We are an organisation full of experienced and motivated individuals. Every day on base offers an embarrassment of riches in terms of enlightening perspective. This is Sydney HEMS after all, and the majority of permanent consultants in the service are actively involved in education.
– Cases are usually volunteered for discussion by participants (as opposed to being selected by the Duty Retrieval Consultant). The emphasis is always on learning, curiosity is celebrated (and practiced even by our most experienced personnel), and the process never feels punitive. I have no doubt it will have taken years to cultivate this level of psychological safety [1], and will also have required great courage to initiate.
– There is buy-in across the organisation. CCPs and doctors. Senior and junior staff. It is highly unusual for C+C not to take place on a given day.
Why do I personally love it so much?
– Never before have I enjoyed the luxury of regular protected time… to talk shop (I absolutely love to talk shop). Again, stark contrast to the hospital environment, where we are so often blitzed with service provision to the point where it’s a challenge to schedule emptying your bladder!
– I crave feedback. I’ve spent my career desperately searching for more of it. C+C provides it on tap. And from multiple perspectives.
– I’m not alone in my feelings here. We all love it. C+C provides the oxygen that fuels high performance in this service.
However… back in October ’22 last year I identified a problem
The learning was staying in the room. If you weren’t there, you didn’t benefit from the education. Particularly early in my year I was desperate to squeeze as much as I could from C+C – but I could only attend so many.
Sure, I could tune in on Microsoft Teams, but it’s a big commitment to do that regularly when not at work, and the audio isn’t perfect – especially when the group chatter is particularly boisterous.
In some sessions I noticed a GoogleForm being filled out by the DRC – an electronic record of cases discussed, with learning points. It took some digging to find out where this record was kept. When I found it, I felt the documentation (if done at all) was largely the bare minimum, and certainly no reflection of the awesome learning conversations taking place.
I believed I had uncovered a problem: suboptimal organisation-wide learning from C+C.
I promptly commenced a QI project.
Analysis of the problem:
First I constructed an Ishikawa diagram – a visual representation of contributing factors to the overarching problem, divided into distinct categories. This helped me strategise in terms of the interventions I might employ to achieve change.

I then designed a Driver Diagram. This illustrated the component parts of the system I was trying to improve. A deeper understanding of the system clarified what elements would be useful to measure and stimulated change ideas.

The Team
I built a team around me. I managed to acquire two very education-centric (and generally brilliant) consultants in Clare Richmond and Natalie May, along with four registrars (Shannon Townsend, Seira Ikeuchi, Raphael Dworkin and Chloe Morgan) and two CCPs (Jackie Buckthought and Jake Tant).
The registrars would later sign up for C+C as a non-clinical portfolio item when this was formally established in 02/2023.
Model For Improvement (MFI)
I was passionate about the problem I’d identified and believed strongly that this work was important. This meant there was a natural urge to take immediate, impulsive action. However, achieving meaningful and sustainable improvement requires a structured implementation strategy.
The MFI is a tried-and-tested framework in healthcare and is recommended by NHS Improvement [2]. I felt it was an excellent fit for this project because multiple change ideas of unknown efficacy had been generated by the Driver Diagram. The MFI framework starts by asking three key questions:
1) What are we trying to accomplish?
2) How will we know that a change is an improvement?
3) What changes can we make that will result in an improvement?
A brief note on the challenge of education-based projects… it’s very difficult to establish attributable benefit
For most medical education interventions, it is highly challenging to demonstrate clear attributable (quantitative) impact on patient-level outcomes or clinician/team performance. These outcomes reflect multiple tangible/intangible contributing factors, and teasing out the precise effect of the educational intervention is essentially impossible.
And so, for this project we made the decision to look solely at process measures that reflected our interventions, as opposed to broader outcome measures. Whilst not perfect, we felt they would signal improvements adequately.
We have written a proposal for a qualitative research project which aims to capture staff perceptions of QIP impact on performance and culture change – this will put much more flesh on bone than the quantitative data we’ve collected. The proposal is being reviewed prior to formal submission for ethics approval at the time of writing this blog post. It is largely the work of Jake Tant (how lucky I feel to have him on the team – a class act). Watch this space.
What are we trying to accomplish?
Our mission is to improve organisation-wide learning from the daily C+C process. We want more staff to benefit from the learning conversations, even if in attendance.
We know this involves improving C+C learning summary documentation standards, and effectively disseminating content across the organisation.
We have established our SMART aim:
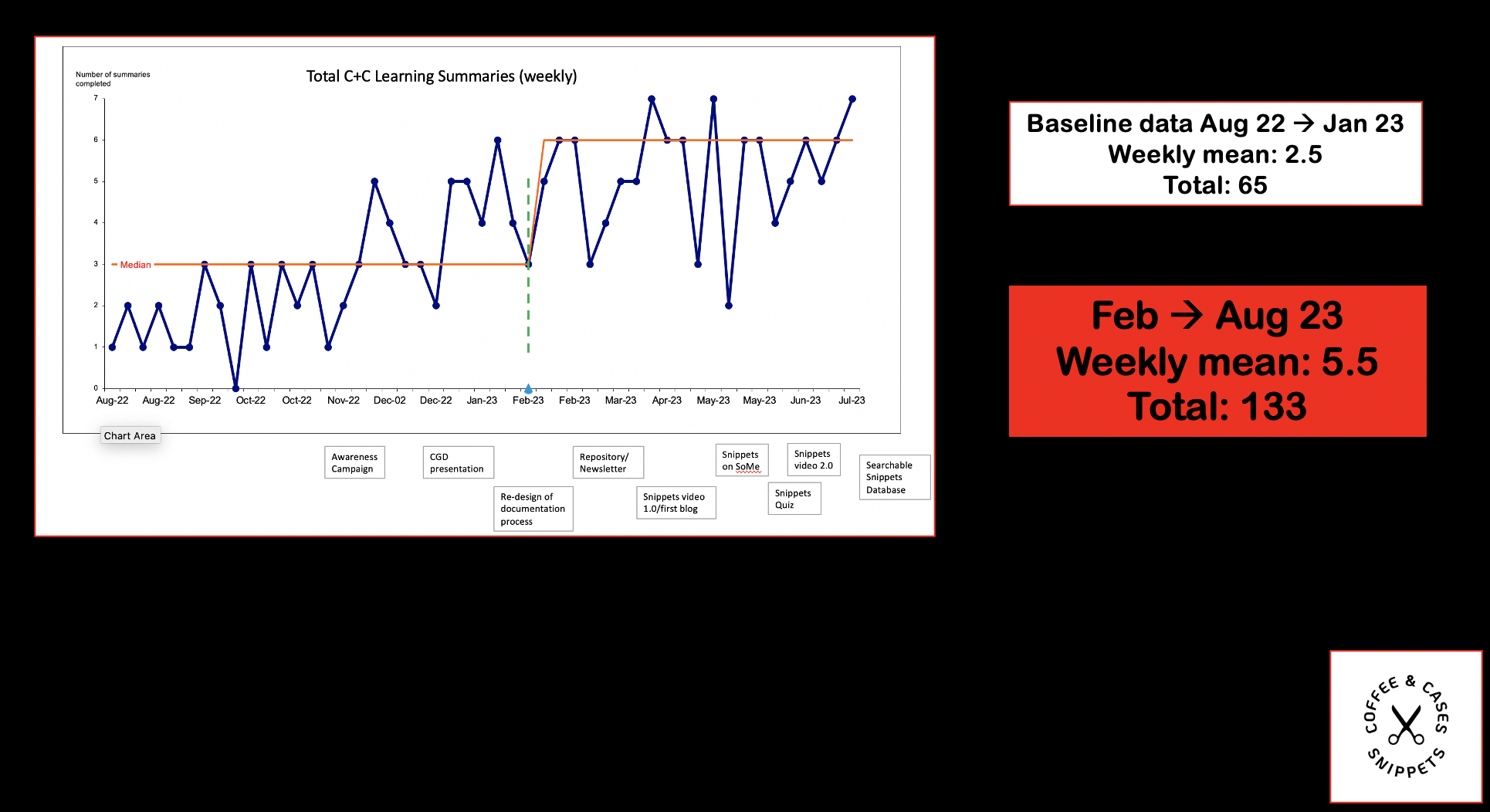
A 50% increase in the total of weekly documented learning points generated by the C+C process by August 2023.
How will we know a change is an improvement?
Outcome measure:
– Total weekly documented learning points
(technically a “process” measure, but directly related to our SMART aim and so labelled our “outcome” measure)
Process measures
– Total weekly completed C+C learning summaries
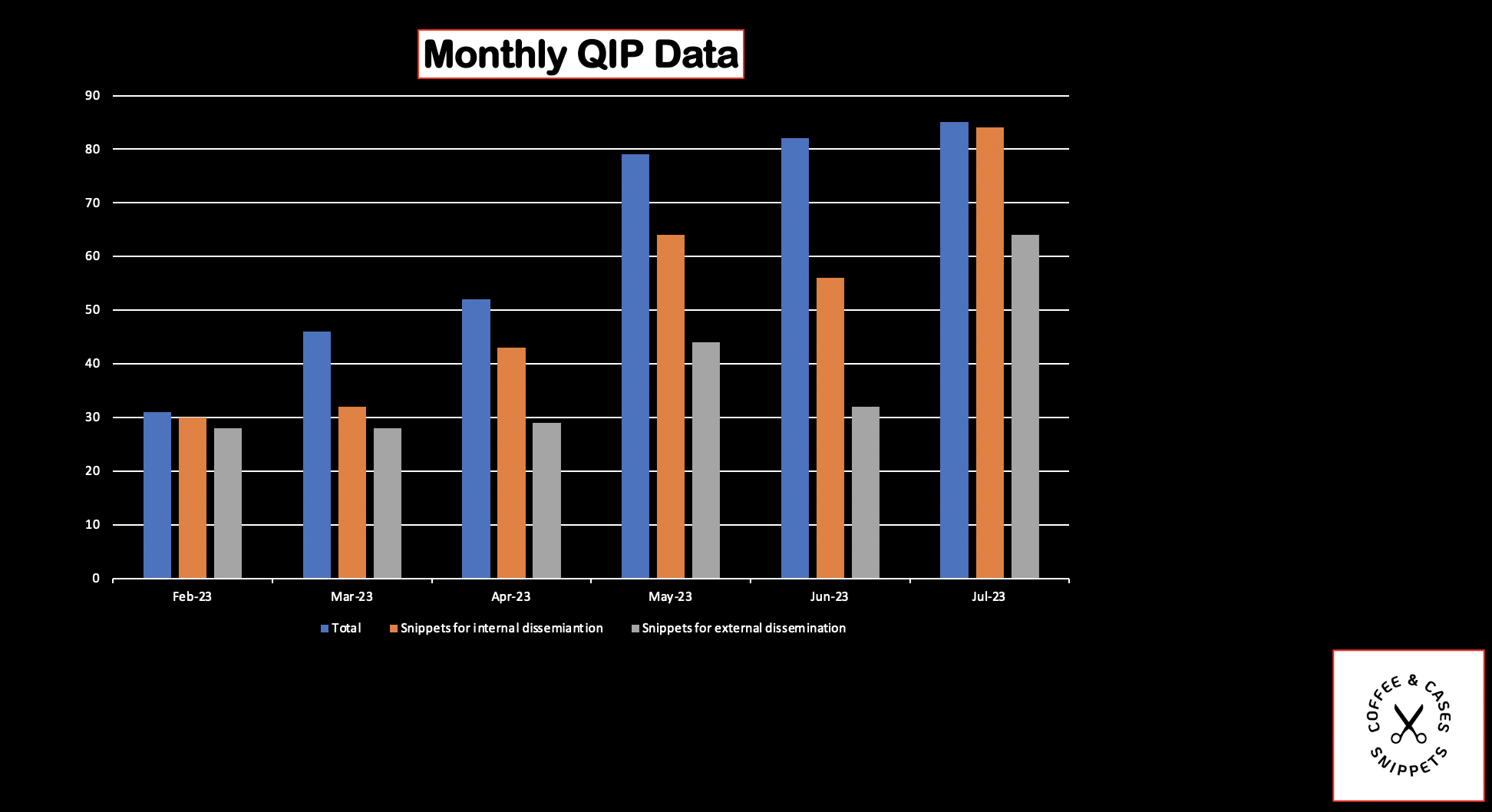
– Total weekly learning points approved for dissemination internally
– Total weekly learning points approved for dissemination externally (social media)
– Social media engagement
What changes can we make that will result in an improvement?
The following change ideas were generated by the Driver Diagram. Those crossed out proved to be unpopular/deemed unnecessary when the project was pitched to the service back in January. However, the rest were instituted which has been rewarding.

New ideas spawned as the project gained momentum. Most crucially, the idea for a C+C learning points repository emerged as I started extracting and finessing discrete learning points from the C+C hard data (from the GoogleForm). This would ultimately pave the way for the searchable database which is being launched at the CGD today.
Baseline Data


Timeline of interventions/actions:
11/2023
– A project awareness campaign was initiated. This consisted of Whatsapp messages and emails from Clare Richmond and myself to the CCP, consultant, and registrar groups.
02/2023
– I presented the QIP plan, baseline data, and proposed timeline at the January ’23 Education Day. This plan has been stuck to.
– The re-design of C+C documentation process was launched. The responsibility of completing the form was shifted from DRC to a registrar (or particularly keen consultant). For a few weeks I made a point of texting the DRC prior to C+C in the morning to make sure they were aware of this change.
– The Googleform was adjusted so it was more prescriptive in terms of how best to fill it in. The hope was this would yield more usable points (i.e. consumable without knowing the context of the case discussed). An instructions email was also sent to all staff.
– C+C was formally established as a non-clinical portfolio, and a C+C Teams file was created which centralised all QIP-related documents.
03/2023
– In March the C+C learning points repository was created. The C+C team began “extracting” learning points from the hard data, and then posting them to a shared document available for the whole service to view. Often, post-extraction editing was required prior to sharing in order to ensure the content wasusable. Increasingly however, content has been lifted straight from the original learning summary form, which reflects an improved understanding of how to document C+C.
– The C+C learning points repository set the wheels in motion for the creation of the searchable database – see below.
– The inaugural C+C monthly newsletter was released at the end of the month.

4/2023
– The C+C “Snippets” brand was born.
In my view, this was the most important moment in the story of this QIP. The word and logo instantly make clear what we are trying to do. I think it also conveys a cool, innovative energy. It instantly caught on. The word Snippets has become part of the Sydney HEMS lexicon, and it is often heard framing C+C discussion – “what Snippets we can take from this case?”.

– The first C+C Snippets rolling slide-deck video went live at Bankstown and Wollongong bases. A single Snippet per slide. Slide change every 30 seconds. Displayed on screens 24 hours a day (if the tech behaved itself)

– April also saw the first C+C-inspired blog post. A total of three posts have been published so far in the C+C Snippets blog series.
Coffee and Cases Snippets: Intubating the patient with a HAGMA
Top 10 Coffee and Cases Snippets from April 2023
Coffee and Cases Snippets: Don’t Leave Me In Suspense
5/2023
– Launch of C+C Snippets on social media. Two tweets per week – all pre-approved by Nat May.


– We initiated formal consultant vetting via excel spreadsheet. All Snippets are now evaluated for appropriateness for internal dissemination, external dissemination (i.e. social media and searchable database). If there is any doubt, a second consultant vetting can be requested.

– We also started tagging content to the PHRM curriculum via the C+C spreadsheet. This process is key for the searchable Snippets database.

6/2023
– I presented the first C+C Snippets Quiz at the June Education Day.

– Launch of the second, new and improved, version of the C+C Snippets video (with inclusion of 1%ers). All content fully vetted (deemed appropriate for internal dissemination). Each slide has a Snippet Unique ID number and QR code to facilitate feedback on the content.


– This Snippets video has been rolled out at Bankstown, Wollongong, Lismore and Newcastle bases.
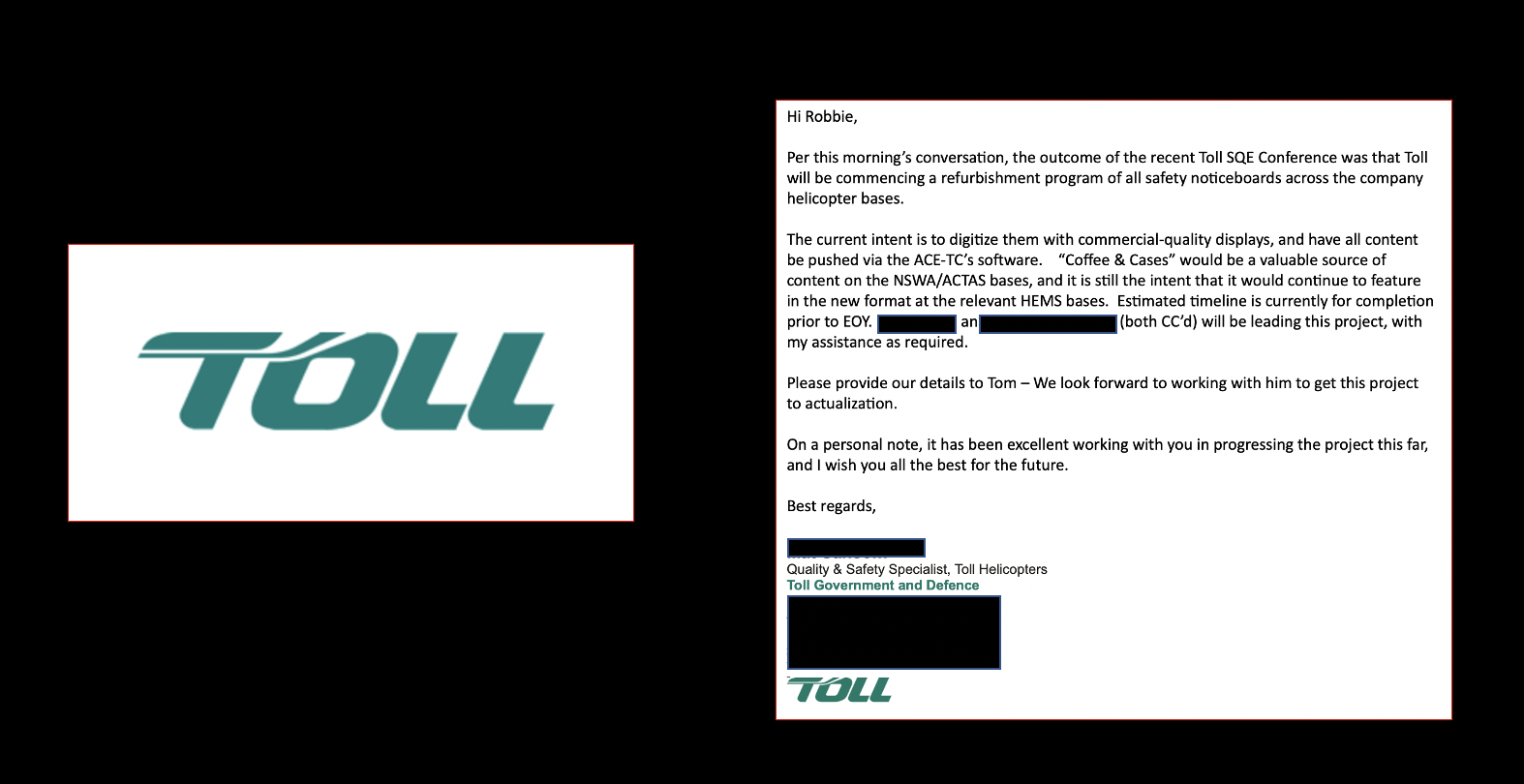
An issue we have encountered is screen availability. I noticed that screens in prominent areas at Bankstown and Wollongong bases lying dormant (switched off, unused) – the Toll noticeboard screens. I saw an opportunity and approached a Toll quality and safety specialist with the idea of playing the Snippets video on these screens across NSW Toll-aeromedical bases. I pitched it as gesture of collaboration between Toll and NSWA. The idea has been presented at an internal quality and safety conference – and subsequently approved by Toll senior management. It is scheduled to be rolled out before the end of the year.
7/2023
As this QIP has evolved, it has emerged that this newly established learning point-processing system (“itemise, vet, disseminate”) is not solely applicable to C+C. I believe it can be applied to all education and governance platforms in this service. And the work has already begun.
The first additional platform to engage has been M+M. It is helpful that I am also on the M+M team and gave the M+M presentation at the June CGD. I planted some subliminal messaging in the presentation…


I pitched the idea of M+M Snippets to consultant leads Sarah Aldington and Ilana Delroy-Beulles who have been enthusiastic and supportive.
There is now an M+M Snippets excel spreadsheet, which follows the exact same process.

Results so far
I’ll just drop the graphs on you – we are comfortably achieving our SMART aim, and demonstrating significant gains across all our measures. The green dotted line is when we started our QIP interventions (other than the awareness campaign) and so I have re-calculated the median from that point.



Additional engagement with @SydneyHEMS Twitter profile:

For the reasons previously described re: the challenge of educational projects, these measures are blunt tools. The qualitative data we plan to collect when given to the go ahead will be far more insightful. However, it is unequivocal that there has been significant improvement in our C+C processes as a result of the QIP.
It is worth noting at this point that we will continue to collect data until the end of August. The reason being the most important intervention has not yet been implemented… until now.
Searchable Snippets Database
https://www.pondermed.com/snippets/
It is currently up on my blog as it will take some tinkering to get it up on the Sydney HEMS website. It is frustratingly slow on my website and will be much faster when eventually migrated over.
The database can be searched by Snippet source (C+C, M+M, 1%ers… hopefully more soon), keyword, and/or PHRM curriculum tag.
My romantic idea is the database might occasionally be utilised whilst en route to a patient (via smartphone) so the team can feel maximally prepared for the mission. However, this should only be considered after consulting the appropriate SOP
Sustainability
This is always the challenge with quality improvement.
A formal handover process has already taken place. Tom Brown is the new C+C registrar lead. Clare and Nat will continue as consultant leads.
I’ve tried to streamline and simplify the new processes as much as possible. The C+C (and M+M) excel spreadsheet, WordPress and Canva are the only pieces of software we’re using. It’s remarkably simple to update the Snippets video and Snippets database – it involves uploading CSV… and then the software does all the hard work. Tom Brown will be overseeing this process.
I am in the process of creating an instructions document and video for the C+C non-clinical portfolio team – these will be available on Teams before I leave. These resources will explain everything.
And I’ll always make myself available to take a call about this project from the other side of the world. It’s been my baby for 8 months!

Thank you everybody for a dream year! I’ll miss you!
Robbie Lloyd
References
[1] Psychological Safety and Learning Behavior in Work Teams
Author(s): Amy Edmondson
Source: Administrative Science Quarterly, Vol. 44, No. 2 (Jun., 1999), pp. 350-383
Published by: Johnson Graduate School of Management, Cornell University
Stable URL: http://www.jstor.org/stable/2666999
[2] Plan, Do, Study, Act (PDSA) cycles and the model for improvement. NHS Improvement. Jan, 2022.


Pingback: HEMS Debrief #5 – Dr Robbie Lloyd | Greater Sydney Area HEMS
Pingback: Coffee & Cases Snippets – August 2023 Newsletter | Greater Sydney Area HEMS