

Source: Pexels.com
By Jess Hegedus
Sydney HEMS recently provided medical teams to attend a number of dance festivals, as part of a NSW Government plan to provide specialist critical care at events where there is a high risk of drug related illness. Along with teams provided by a number of NSW Health emergency departments, NSW Ambulance paramedics and other services, our teams provided advanced critical care interventions on-site to numerous patients. This was a fantastic team effort, and it was suggested that without this effort, a number of these patients may not have survived or may have suffered serious neurological morbidity.
More details here: https://www.theguardian.com/australia-news/2019/jan/28/man-on-life-support-after-suspected-drug-overdose-at-sydney-music-festival
We’ve had much discussion on base over the last few weeks about the planning involved and potential management issues that might arise at such events. This has been a great opportunity to consider more broadly the pre-hospital management of patients presenting with toxicity following illicit drug use.
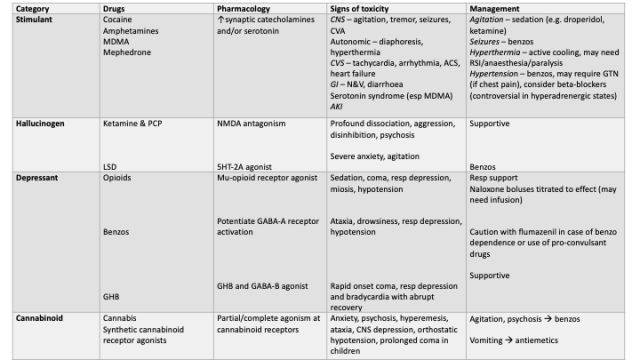
Broadly, toxicity from illicit drug use can be divided into 4 syndromes. Whilst the patient, or those accompanying them, may not be able to provide specifics on the substance/s consumed, appropriate management can often be guided by characteristic signs of toxicity. Some more information about different drug classes, their presentation and management is provided in the table below (adapted from Anderson 2017, incorporating the other references listed below).
The remainder of this brief review will focus on stimulant associated toxicity, which is commonly seen in these settings. In these patients, serious toxicity can occur acutely via a number of systemic effects. The sympathomimetic actions can create a hypertensive crisis, resulting in intracranial haemorrhage, and cardiac ischaemia or arrhythmias. Hyperthermia is an extremely common presenting symptom, particularly with methamphetamines (most commonly with MDMA), with extreme hyperthermia usually present in fatal overdoses from these agents. The exact mechanism underlying hyperthermia from these agents is uncertain, and likely multifactorial, and it is exacerbated by other drug effects (e.g. agitation, seizures) and the environment in which they’re taken, such as hot and humid conditions during Summer festivals or in clubs. Hyperthermia in this context may also be part of a presentation of serotonin syndrome, as some stimulant agents (e.g. MDMA) increase synaptic serotonin levels. Serotonin syndrome may develop within minutes to hours and is characterised by a triad of autonomic effects (e.g. hyperthermia, tachycardia), muscular hyperactivity (e.g. clonus) and neurological symptoms (e.g. agitation). Ultimately, significant hyperthermia requires urgent management, and can result in a 13-fold increase in mortality at temperatures greater than 39.5 degrees (Walter and Carraretto 2015). Other serious complications of hyperthermia include cerebral dysfunction (possibly exacerbated by direct drug effects), seizures, rhabdomyolysis, AKI and coagulopathy.
The management of stimulant toxicity is largely supportive, with early treatment of agitation and psychosis often required to facilitate further management. When non-pharmacological methods are unsuccessful, parenteral agents are usually required in the pre-hospital setting. Antipsychotic agents are often administered as a first line agent, and are particularly useful when the cause of agitation is unknown, with droperidol (a butyrophenone antipsychotic) available for use by NSW Ambulance paramedics.
The advantage of these agents are that they are relatively safe, with a low incidence of respiratory depression and an intubation rate of 4% reported in the literature (Richards, systematic review). A study of methamphetamine-affected patients presenting to a tertiary ED in Brisbane reported adequate sedation in 87% of patients receiving IM droperidol, with a further 8% increase in efficacy following a further dose (Isoardi et al. 2018). Duration of action is reported as 80 – 120 minutes in the literature, usually sufficient for pre-hospital transport without further dosing (SR). Disadvantages include a risk of extra-pyramidal side effects and QT interval prolongation, along with a relatively longer onset of action (may require 15-25 minutes for effect) compared with other agents. Another commonly used parenteral agent for undifferentiated agitation is the benzodiazepine midazolam, however the efficacy of this agent appears to be more variable and difficult to titrate in these settings. The incidence of both under- and over-sedation were reported as more frequent in the literature, with a well documented risk of paradoxical agitation with midazolam.
Ketamine (both IM and IV) has emerged as a useful agent to manage agitation in the prehospital setting, and is successfully utilised by our service. Advantages of this agent are a low risk of compromised airway reflexes or respiratory drive and a predictable, rapid onset by IV or IM injection. Isoardi et al. (2018) reported ketamine as providing successful sedation in the small number of patients in whom droperidol did not, and other sources have reported ketamine as more effective than droperidol, midazolam and the combination of the two (Gottlieb et al. 2017). Potential disadvantages include a risk of emergence delirium and a shorter duration of action (reported as 5-30 minutes), compared with droperidol, and may therefore require re-dosing in the prehospital setting. Furthermore, ketamine may result in a catecholamine surge causing hypertension, which may theoretically worsen hypertension seen in hyperadrenergic states (e.g. following cocaine overdose). However, hypertension and tachycardia seen following ketamine use is usually brief and there has been no evidence that this effect is significant.
Whilst a review of the management of amphetamine toxicity (Richards et al. 2015) reported further studies are needing assessing the utility of ketamine sedation in amphetamine toxicity, there is a reasonable volume of literature assessing ketamine use in undifferentiated agitation which can guide its use in this setting. A systematic review published in 2018 (Mankowitz et al. 2018) has analysed the use of ketamine for undifferentiated agitation in the pre-hospital and ED setting, with a total 650 patients included. They reported adequate sedation following IM ketamine in a mean time of 7.2 minutes following a mean IM dose of 315mg or 4.9mg/kg. The most common side effects were hypertension and hypersalivation, with other reported side effects being vomiting, emergence delirium and, uncommonly, transient hypoxia and laryngospasm. The intubation rate following ketamine administration was reported at 30.5%, however this was mostly associated with pre-hospital use and is suggested that intubation was the likely clinical course in these cases. The intubation rate in the ED was 1.8% and 4.9% in aeromedical transport.
Another important management consideration in amphetamine affected patients, is the management of temperature. There is no determined safe level of hyperthermia in stimulant toxicity, and patients should be actively cooled using an escalating approach depending on their level of hyperthermia. Basic interventions include moving to a cool environment, misting with water and administration of cold IV fluids. Some patients will require ice pack application, sedation, progressing to RSI, anaesthesia and paralysis to reduce heat generation. Antipyretics are not useful as the hyperthermia is driven by excessive heat generation due to the stimulant drug, rather than an alteration in their hypothalamic set point.
References:
Anderson, M. (2017). Poisoning with illicit drugs. Paediatrics and Child Health. 27.
Gottlieb, M. et al. (2017). Approach to the agitated emergency department patient. Journal of Emergency Medicine, 54 (4)
Isoardi, K. et al. (2018). Methamphetamine presentations to an emergency department: Management and complications. Emergency medicine Australasia
Mankowitz, S. et al. (2018). Ketamine for Rapid Sedation of Agitated Patients in the Prehospital and Emergency Department Settings: A Systematic Review and Proportional Meta-Analysis. The Journal of Emergency Medicine, 55.
Matsumoto, R. et al. (2014). Methamphetamine-induced toxicity: An updated review on issues related to hyperthermia. Pharmacology & Therapeutics,144.
Richards, J. et al. (2015). Treatment of Toxicity from Amphetamines, Related Derivatives, and Analogues: A Systematic Clinical Review. Drug and alcohol dependence, 150
Walter, E., & Carraretto, M. (2015). Drug-induced hyperthermia in critical care. Journal of the Intensive Care Society, 16(4), 306-311.

