The October CGD involved discussion of several outstanding examples of prehospital trauma care provided by teams within our service. These were explored by Dr Karel Habig in his ‘Learning from Excellence’ presentation and Dr Chris Partyka, Chris Wilkinson (critical care paramedic) and Dr Simon Keane in a review of major trauma cases requiring prehospital activation of the code crimson pathway. We use this pathway to provide rapid, streamlined transfer to definitive care, for exsanguinating haemorrhage that is refractory to standard resuscitation (more info here: https://www.aci.health.nsw.gov.au/networks/itim/clinical/trauma-guidelines/Guidelines/trauma-code-crimson-pathway).
Part of the code crimson guideline is a reminder of the importance of optimal prehospital trauma care and there were several useful discussion points, throughout the day, about the prehospital management of these patients.
- Point of care ultrasound (POCUS)
The group considered the benefit of utilising US on scene for initial assessment and stabilisation vs. concerns that it may increase scene time in a patient who requires transfer to definitive care. Our US audit team reported that GSA HEMS data suggests that the use of POCUS adds between 0-6 minutes to scene time. They suggested that in most cases it is appropriate to do a quick lung US to check for pneumothorax on scene, followed by the rest of the eFAST scan en-route to hospital. The use of eFAST is highlighted in the Code Crimson guideline, and in the prehospital setting can allow early identification of likely bleeding source to facilitate rapid transfer to the correct intrahospital location and involvement of the correct teams.
Another use of POCUS discussed was the identification of injuries that may be amenable to prehospital intervention to allow early consideration of potential issues that may arise during transport. Awareness of a problem allows the team to team to pre-brief, prepare equipment and mark the patient, if required. They may benefit from the opportunity to talk through and/or mentally rehearse the procedure and consider access and logistics issues early.
- Pre-RSI stabilisation
Another discussion was around the importance of optimising patients prior to RSI. This can be difficult in the prehospital setting, with limited people to perform interventions and will require careful consideration of the appropriate order of interventions to ensure this. This may involve some time spent on resuscitation prior to RSI, consideration of procedures or management of agitation with judicious use of sedation to allow pre-oxygenation and usual preparation (i.e. delayed sequence intubation).
- Communication and coordination of care
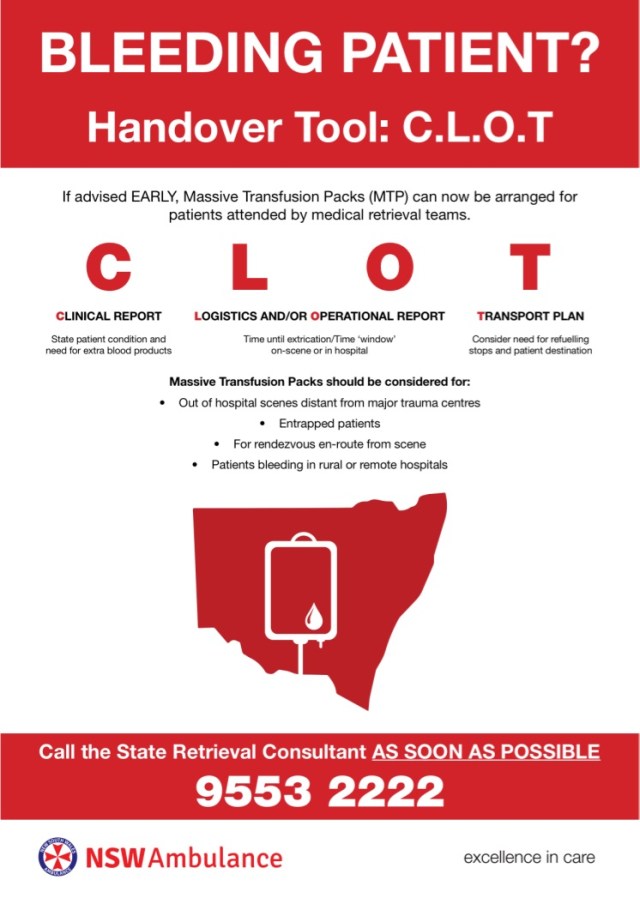
We have multiple protocols that may be required in tandem with the code crimson guideline, such as a prehospital massive transfusion protocol (MTP), which can facilitate the delivery of blood products to the retrieval team en-route to hospital. These protocols work well when there is rapid identification of exsanguinating haemorrhage and early communication to allow for logistical coordination. Our MTP protocol suggests considering activation for scenes distant from major trauma centres, entrapped patients, rendezvous on route from scene, or patients bleeding in rural and remove hospitals. The below poster summarises the process that our teams can utilise to arrange prehospital MTP activation. The use of the code crimson guideline and prehospital MTP have contributed to good patient outcomes, and highlight the benefit of clear early communication between different teams, applying organised processes within an integrated trauma service.
Further discussion was the regarding the effective use of communication within well-functioning teams. Chris Wilkinson described an excellent example of team communication as everything being “heard, visualised and discussed” between them. This allowed them to maintain a shared mental model and overview of the situation whilst they were independently managing multiple time critical tasks and maintaining momentum to definitive care. This was a great reminder that this continuous, open communication is what we should be aiming for in our teams.
The next CGD will occur on 31/10 – please see flyer below.
MTP protocol C.L.O.T handover tool: