
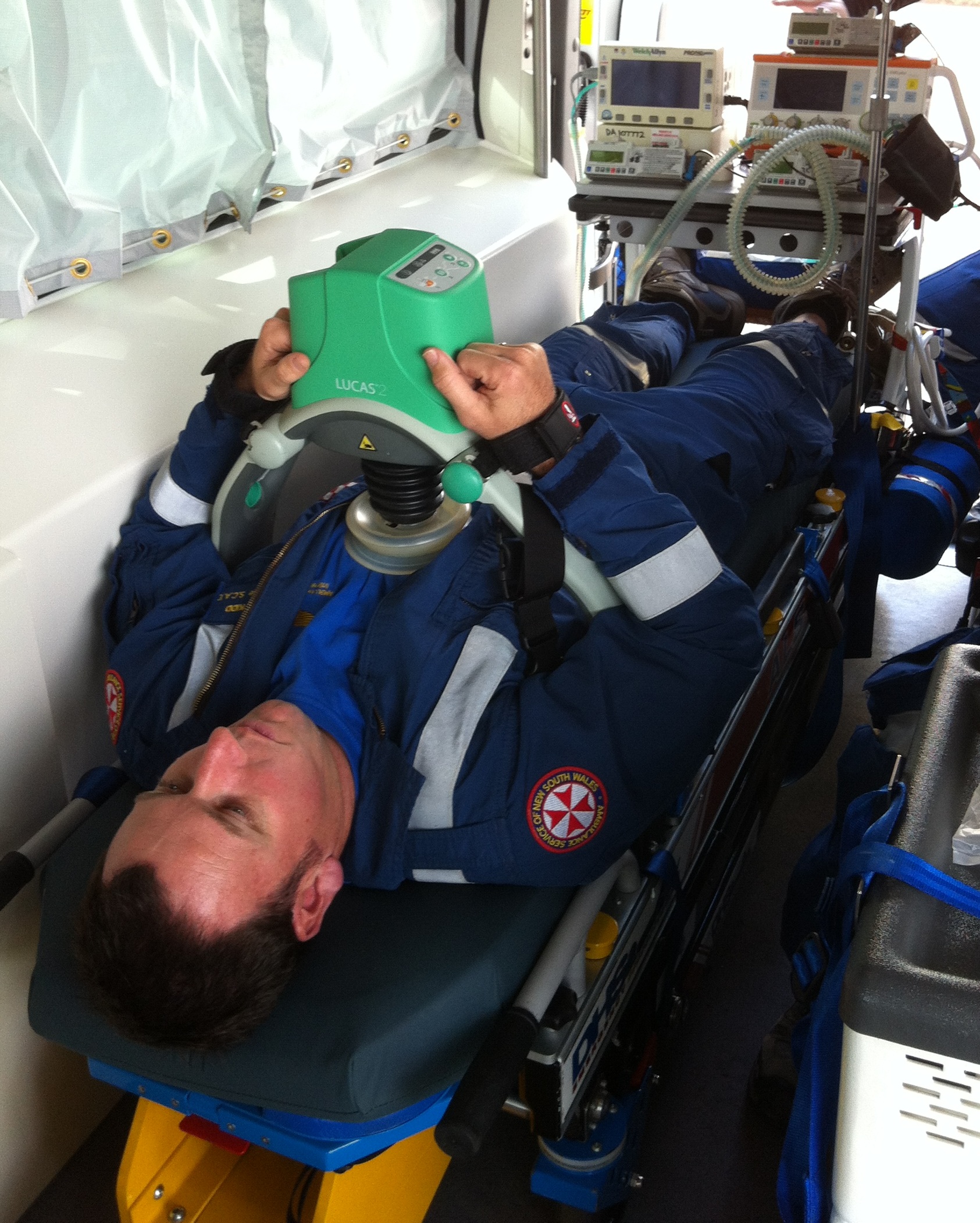
Today we commenced trialling and training with the Lucas 2 automatic chest compressor device.


First it was formally introduced to our consultant Lucas Fox who had been concerned at talk around the base that ‘Lucas’ would be involved in a lot more jobs from now on…then we ascertained its fit both within our retrieval road vehicles and around the chests of our most thoracically gifted paramedics.

Now to see if it works as a helpful adjunct to our regular resuscitation of the arrested heart.
Scenario – 57 yr old man, collapsed on road whilst walking his dog. Road crew in attendance, patient in VF arrest, no pads on yet, CPR and being bagged with BVM.
Scene/Patient/Challenge – Team arrived, confirmed VF arrest and instigated defibrillation. Paramedic applied Lucas 2 while doc secured airway and instructed road crew to obtain IV access and administer drugs. Lucas paused at 2 minutes to observe rhythm and patient defibrillated back into NSR.


Learning points from debrief for clinical practice :
1. Effectiveness of Lucas 2 in providing cerebral and pulmonary perfusion. Patients have been known to regain consciousness and require sedation despite having no intrinsic cardiac output. It also renders ETCO2 as a prognostic tool in cardiac arrest useless.
2. Who should do what? It was generally felt that the paramedic should be the one applying the device whilst the doctor takes handover, attends the airway etc but this may need to be protocolled.
3. Dimensions/practicality: it was possible to intubate the mannequin without the laryngoscope handle butting the device. The device also fits into the road ambulance as long as the back board sits above the stretcher sides.
Team: Geoff Healy (doc), Bob Lisle (para), Dave Kidd (road crew), Digby Horne (road crew), Helen Ellis (STAR), Brian Burns (SRC), Cameron Marks.


OK, quick Q’s
(i) patients’ arms – do you use the velcro straps to have arms up & secured to the device? If so, how easy is it to get IV access with arms in this position? or do you just whack in an IO?
(ii) I have very sceptical colleagues. They tell me ‘not proven to deliver better outcomes than manual compressions’ which seems odd given better effectiveness (perfusion) with the device. Any data showing improved survival to discharge with the device?
Ain;t going to get these in country practice anytime soon – but may be benefit for austere / Antarctica where limited person power to deliver CPR and potentially prolonged periods of CPR (espec hypothermic)…
Grateful for your comments…
Sorry Tim only just noticed this comment.
(i) Yes. Whenever we’ve used this for real the iv has usually already been placed by initial rescuers, but I would imagine it would be difficult, so yes IO followed by quick CVC or EJV would make sense.
(ii) Sadly not yet, but makes staff injuries less likely, patient is easier to transport, CPR is more effective, and a member of the team is freed up.