
This week on the HEMS base, our fearless Supervisor of Training, Dr Cliff Reid has again proven himself willing to go above and beyond in the name of medical education. This time by asking to be fibreoptically intubated.

 So how does a day proceed from a discussion of cases over morning coffee to intubating a colleague? Our daily “Coffee and cases’’ review discussion led to a review of the Advanced Airway Currencies and a discussion of the kit available. This, in the interests of increasing the fidelity of our simulation, resulted in Dr Reid requesting to be intubated. For those of you that know Cliff, this will probably not come as a surprise! Exhibiting the true spirit of the FOAM community, Dr Reid had his intubation filmed and has posted it along with an account of his experiences here: http://resus.me/awake-intubation/
So how does a day proceed from a discussion of cases over morning coffee to intubating a colleague? Our daily “Coffee and cases’’ review discussion led to a review of the Advanced Airway Currencies and a discussion of the kit available. This, in the interests of increasing the fidelity of our simulation, resulted in Dr Reid requesting to be intubated. For those of you that know Cliff, this will probably not come as a surprise! Exhibiting the true spirit of the FOAM community, Dr Reid had his intubation filmed and has posted it along with an account of his experiences here: http://resus.me/awake-intubation/
The Advanced Airway Equipment is kept in our interhospital packs and consists of both a videolaryngoscope (The King Vision) and a bronchoscope (the Ambu aScope2).

It also includes a quick guide to the use of both and a call and response Awake Intubation Checklist. Below is our advanced airway algorithm as taught to all new registrars.
 The King Vision scope is a self-contained video-laryngoscope with 2x size #3 sterile blades and a reusable screen. It is anticipated that it will be used in interhospital missions to intubate any patient that has features predictive of a difficult airway. However, there are a few important points to note about its use. Firstly, insertion requires that the patient be able to open their mouth at least 18mm. The screen and blade can become disconnected, resulting in freezing of the screen. Gently pushing the two back together will fix the problem. Similar to other videoscopes, the King Vision is inserted in the midline rather than from the right-hand side of the mouth and the blade can be inserted either into the vallecula or used to lift up a large epiglottis.
The King Vision scope is a self-contained video-laryngoscope with 2x size #3 sterile blades and a reusable screen. It is anticipated that it will be used in interhospital missions to intubate any patient that has features predictive of a difficult airway. However, there are a few important points to note about its use. Firstly, insertion requires that the patient be able to open their mouth at least 18mm. The screen and blade can become disconnected, resulting in freezing of the screen. Gently pushing the two back together will fix the problem. Similar to other videoscopes, the King Vision is inserted in the midline rather than from the right-hand side of the mouth and the blade can be inserted either into the vallecula or used to lift up a large epiglottis.
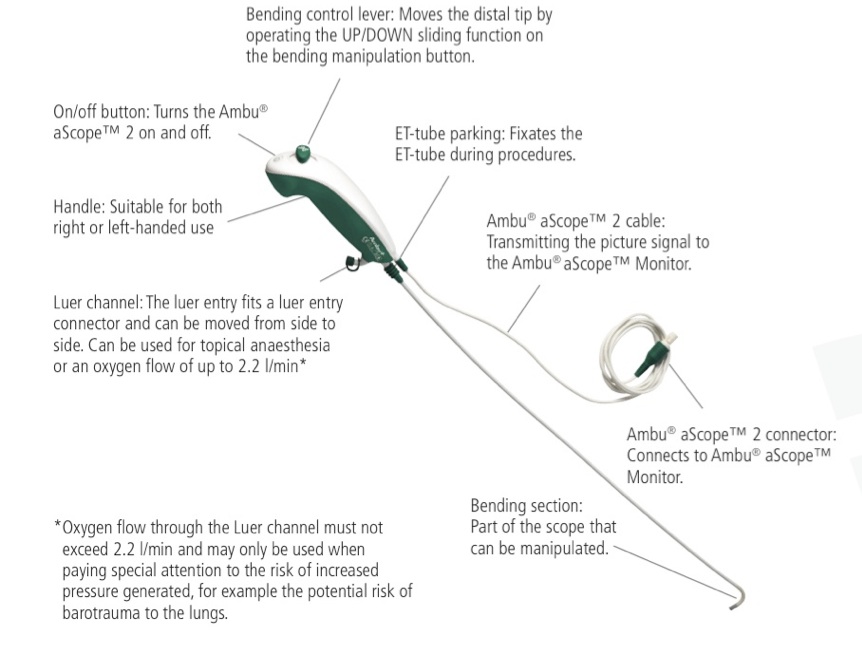
The Ambu-aScope is also a really interesting piece of kit and one that is definitely worth playing with, especially for those who haven’t done bronchoscopies, nasendoscopies or AFOIs in the past. The aScope pack consists of a re-usable screen with an AC adaptor and 2x disposable sterile scopes. The scopes themselves have a luer channel, however it is too small (<1mm diameter) for use as a suction port. The channel can be used to administer local anaesthetic in a ‘spray as you go’ approach, administering oxygen or for flushing with air to blow any debris / mucous off the camera at the tip. Unlike traditional fibreoptic scopes used in theatre, the Ambu aScope is a camera tipped scope without inline fibreoptic cables. Therefore there is less risk of damaging the scope itself with twisting and turning during insertion. I was also quite impressed with the picture, given that it is a single use item.

There are two main situations in which the Ambu scope is likely to be used in the retrieval medicine environment.
- A true awake fibreoptic intubation in a patient in whom videolaryngoscopy or LMA insertion is not possible. For example, in patients with limited mouth opening or significant supraglottic swelling (eg trismus or Ludwig’s angina). This is the situation we will be discussing here.
- In the rescue airway situation where an LMA has been placed and a scope can be use to improve accuracy of ETT placement. With a traditional scope the ETT could be preloaded and railroaded over the scope once it is through the cords. This is possible with the aScope but would require some gentle advancement of the scope and tube together before the scope came out the end of the LMA as the aScope is significantly shorter than a traditional scope. It has been suggested that the aScope could be passed into the cords with visual confirmation and then cut and used as a traditional bougie but this would then prevent visual confirmation of ETT placement into the trachea.
This was a fascinating exercise for many reasons. Firstly it shows that it is possible to scope and intubate an awake patient (many thanks to Cliff!) with no other sedation on board. Secondly it was very useful for us, both paramedics and doctors, to have the opportunity to use the equipment we have in the kit. For the sake of the exercise, I was under strict instructions to stick to what is available in the kit alone. Of note we did not pre-treat with an anti-sialagogue (as Cliff had to drive home and didn’t want the blurred vision!). Excessive secretions weren’t an issue, apart from when he cried. SO…..DID IT WORK? Yes. Overall it was a great success! Cliff tolerated examination of his nasopharynx cords and trachea down to the carina and tolerated the nasal placement of a 6.0 reinforced ETT, all with topicalisation alone. However he experienced significant discomfort in his posterior nasopharynx and sinus, which suggested that the topicalisation of this part of his airway was insufficient.


HOW IT WAS DONE – using only kit available in the Advanced Airway pack.
- Co-phenylcaine spray to the nose for both topicalisation and vasoconstriction. We started with 3 squirts/nostril as per the Advanced Airway protocol however needed to add approx. 3/nostril more. As co-phenylcaine is 5%, 1 squirt (0.1ml) is 5mg. It is very important to use the correct nozzle with the bottle as it then gives a correctly calibrated dose.The other advantage to co-phenylcaine is the vasoconstriction it produces. Despite a number of passes of the scope and scope + tube, there was no bleeding from Cliff’s nose.
- Nebulized 2% lignocaine. In a compliant patient (such as Cliff!), ask the patient to take deep breaths and nebulize to an end point of a change in voice (indicating anaesthesia of the vocal cords).
- Spray 1-2mls of 2% lignocaine (20mg/ml) to the back of the tongue using a 3ml syringe and a blunt drawing up needle.
OTHER EQUIPMENT, NOT IN OUR PACK THAT WE LATER USED (so we could put the ETT in!)
- Mucosal atomizer device (which we stole from the nasal fentanyl pack). This was a short MAD device, enabling topicalisation of the anterior but not the posterior part of the nose. Using a MAD device with a longer nozzle (a commercially available item) may have assisted this.
- Oxygen tubing and a 3 way tap. A tried and true method for tropicalizing in theatre, this may prove to be an effective addition to the interhospital pack.
LEARNING POINTS :
- AFOI is a slow process. From unpacking the kit it took just over 2 hours to intubate Cliff (admittedly we were going slowly and started with the scope alone). Whilst in experienced hands, using familiar kit in an environment set up for it, AFOI can be done relatively quickly. If a true AFOI is being done by our service it is likely to be being done in a patient with a difficult airway, in a small hospital where staff are unfamiliar with the procedure (therefore we need be completely self sufficient) and possibly by someone who has never done one before. Therefore it is vital that we all become as familiar with the kit as we can be.


- Adequate topicalisation is the key and the posterior nasal cavity is notoriously difficult to anaesthetize. The trick is to ensure adequate contact time between the lignocaine and the mucosal surface. Merely spraying into the nose doesn’t topicalise the posterior nasopharynx as the liquid will just run down the back of the throat. In Cliff’s case this is exactly what happened. Despite spray and some nebulization, he still had significant discomfort (OK pain) in the posterior nasopharynx which he described as significant sinus pressure (‘My face is going to explode!!’). However, once we got the scope down the nose to the cords, he didn’t require any extra topicalisation (though we gave some anyway) and the trachea/carina was sufficiently topicalised to ablate the cough reflex (scope + tube did produce some coughing). Limiting our topicalisation to what was available proved challenging! Co-phenylcaine to the nose seemed to adequately prevent epistaxis but provided inadequate topicalisation. As our patient himself notes on his own blog http://resus.me/awake-intubation/
“The biggest learning point for me was how hard it was to anaesthetize the posterior part of my nasal cavity and nasopharynx. I thought the worst part would be any stimulation of my vocal cords or trachea with lidocaine or instrumentation but this was really fine. Nebulized 2% lidocaine (the strongest concentration we have), atomized lidocaine and co-phenylcaine weren’t sufficient. I can see why people use pastes or gel to maintain mucosal contact while the lidocaine take effect, but we don’t have those (yet).”
- How to improve this? Options that are commonly used in theatre act to increase contact time by either breaking the lignocaine into small particles via a nebulizer (more than we used), a 3 way tap with oxygen tubing or a DeVilbiss atomizer1. Precoating the ETT with lignocaine jelly/crème and placing it in the nasal mucosal works to topicalise the airway and acts as a conduit to pass the scope. Anaesthestists will often coat a pre-cut nasopharyngeal airway with lignocaine jelly and then use it as a conduit in the same way. The longitudinal cut down the NP allows it to be peeled off the scope as it is removed. This would be an option for our protocol but if simplicity is the key then coating the outside of the ETT itself with lignocaine jelly (either straight lignocaine or the lignocaine/chlorhexidine combination used for catheter insertion) would be as good an option. The other advantage of having a conduit is that it greatly simplifies passage of the scope through the nasopharynx and the scope exits the ETT just above the cords, again simplifying its passage.
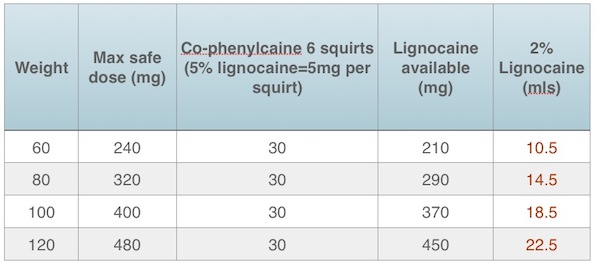
- Dosages. The British Thoracic Society Guidelines on flexible bronchoscopy state the safe maximum dose of lignocaine is flexible bronchoscopy state the safe maximum dose of lignocaine is 8mg/kg2. However, our service has recommended the more conservative value of 4mg/kg be used. This is in part because if a patient is requiring a true awake intubation due to airway difficulty, it is likely being done in a small or remote facility where lipid rescue for local anaesthetic toxicity may not be available. However 4mg/kg is very conservative and may not allow sufficient volume of lignocaine to ensure adequate topicalisation. Practically, it means that we need to think about the most effective method to tropicalize as we have relatively less to work with than we might otherwise wish. We estimated Cliff’s weight at 80kg and used 5mg/kg as the safe dose limit.
- Throughout this sometimes lengthy process it is vital to keep a close eye on the patient for any signs of airway deterioration. Patients with immediate need for airway management are unsuitable for awake techniques. And plans may need to be made for a primary surgical airway.
LINKS/REFERENCES
1 – http://www.jedmed.com/products/atomizer-devilbiss-163.
Written and photographed and anaesthetised and ‘scoped by Dr Emily Stimson – ASNSW Registrar


Did it manage to stop Cliff talking? 😉 Seriously, well done, Cliff and team.